

Abstract
Keywords: Diabetic foot, infection, causative pathogens
Introduction
Diabetes mellitus is a major global health concern whose prevalence continues to increase steadily. One of its most serious complications is the development of foot ulcers, which represent a substantial cause of morbidity among affected individuals. Worldwide, a diabetes-related foot ulcer develops every 1–2 seconds, and a major amputation attributable to these wounds occurs approximately every 20 seconds (1). Among diabetes-related complications requiring hospitalization, diabetes-related foot infections remain the most common and continue to be the leading cause of lower-extremity amputation (2). Follow-up data from patients with diabetes-related foot infections indicate that, after 1 year, only 46% of ulcers have healed (with 10% of these subsequently recurring). In contrast, 15% of patients have died, and 17% have required lower-extremity amputation (3). These outcomes underscore that timely and appropriate infection management remains one of the most critical challenges in this patient population.
The spectrum of microorganisms responsible for diabetes-related foot infections can often be anticipated based on specific clinical factors. Superficial and mild infections are predominantly caused by Gram-positive bacteria, whereas advanced infections are more frequently associated with Gram-negative organisms; in cases accompanied by gangrene, anaerobic pathogens must also be considered (2,4). Particularly in advanced infections, Gram-positive, Gram-negative, and anaerobic organisms may coexist in a polymicrobial pattern (4). Moreover, interactions among these pathogens are clinically important, as they are associated with biofilm formation and the development of antimicrobial resistance (5).
In the absence of a life-threatening infection, the preferred approach is not to initiate empirical antibiotic therapy immediately, but rather to obtain appropriate tissue specimens and await microbiological results before selecting targeted antimicrobial treatment. Conversely, when a life-threatening infection is present, prompt empirical therapy should be initiated based on the most likely pathogens (6). When selecting empirical antibiotics, several factors must be carefully considered, including the availability of previous culture and susceptibility results from the same wound, the clinical severity of the infection, potential adverse effects of the selected agent, the need for dose adjustment according to renal and hepatic function, possible drug-drug interactions (particularly relevant given the high burden of comorbidities and concomitant medications in patients with diabetes), and overall treatment cost (7). In addition, knowledge of the regional distribution of causative pathogens, derived from prior studies, can substantially increase the likelihood of successful empirical therapy. For this reason, studies reporting the local microbiological profile of diabetes-related foot infections are of considerable importance, as they provide clinicians with essential data to guide treatment decisions.
The present study aimed to determine the distribution of causative pathogens among patients with diabetes-related foot infections treated as outpatients or inpatients at a secondary care hospital.
Materials and Methods
Study Design and Patient Selection
This retrospective study included patients who presented to the outpatient clinic or were hospitalized with a diagnosis of diabetes-related foot infection between May 1, 2025, and February 1, 2026.
Patients were eligible for inclusion if they met all of the following criteria:
- Age ≥ 18 years.
- Presentation to our hospital with a diagnosis of diabetes-related foot infection between May 1, 2025, and February 1, 2026.
- A diagnosis of infection was established according to the criteria defined by the International Working Group on the Diabetic Foot (IWGDF), including local signs of infection (swelling, erythema, increased local temperature, pain, purulent discharge) or systemic findings.
- Availability of tissue or aspiration samples obtained from the wound and sent to the microbiology laboratory for analysis.
- Availability of complete clinical and laboratory data in the electronic medical records.
Patients were excluded if they met any of the following criteria:
- Age < 18 years.
- Absence of tissue or aspiration sampling from the wound site.
- Incomplete or erroneous clinical or laboratory data.
- Presence of infections or foot lesions other than diabetes-related foot infections.
The study was approved by the Non-Interventional Clinical Research Ethics Committee of Aydın Adnan Menderes University Faculty of Medicine on March 26, 2026, with decision no. 2026/117.
Definition of Diabetes-related Foot Infection
The diagnosis of diabetes-related foot infection was established according to the criteria defined in the IWGDF guidelines (4). According to these criteria, infection was diagnosed in the presence of local signs of inflammation—such as swelling, erythema, increased local temperature, and pain—or systemic findings including fever, leukocytosis, and elevated C-reactive protein levels. The presence of purulent discharge from the wound and the clinician’s judgment that the lesion was infected were also considered diagnostic criteria.
Surgical Sampling Procedure
Under sterile conditions, any necrotic tissue present in the wound area was debrided using appropriate surgical techniques. Following adequate debridement, an adequate tissue specimen was obtained from the infected area and transported to the microbiology laboratory under sterile conditions for further analysis.
Microbiological Analyses
From the prepared fluid suspension of the specimen, 0.05 mL was inoculated onto 5% sheep blood agar and MacConkey agar plates using a sterile loop under aseptic conditions. The inoculated plates were incubated aerobically at 35°C and examined for microbial growth after 24 hours. If no growth was observed, the plates were re-incubated and reassessed at 48 hours post-inoculation.
Bacterial identification was performed using conventional biochemical methods. Upon detection of microbial growth, isolates were initially evaluated by Gram staining. Gram-negative organisms were identified based on standard biochemical characteristics, including glucose, sucrose, and lactose fermentation; citrate utilization; motility; urease and indole production; ornithine decarboxylase activity; and oxidase reaction. Gram-positive organisms were identified according to catalase activity, hemolytic patterns, coagulase production, susceptibility to optochin, bacitracin, and trimethoprim-sulfamethoxazole, as well as growth on bile esculin agar and in media containing 6.5% sodium chloride.
Antimicrobial susceptibility testing was performed and interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. Identification of methicillin-resistant Staphylococcus aureus (MRSA) was performed using the cefoxitin disk diffusion method in accordance with EUCAST criteria. Each infection episode was analyzed as an independent event.
Results
A total of 197 patients were included in the study. Of these, 137 (69.5%) were male, and 60 (30.5%) were female. During the study period, 11 patients experienced a second infection episode. Overall, 208 wound specimens were obtained. No microbial growth was detected in 12 samples. Among the culture-positive specimens, 38 (18.3%) yielded two distinct infectious agents, indicating polymicrobial infection. In total, 196 culture-positive samples yielded 230 microbial isolates. Of these, 109 (47.4%) were Gram-positive organisms, and 119 (51.7%) were Gram-negative organisms (Table 1).
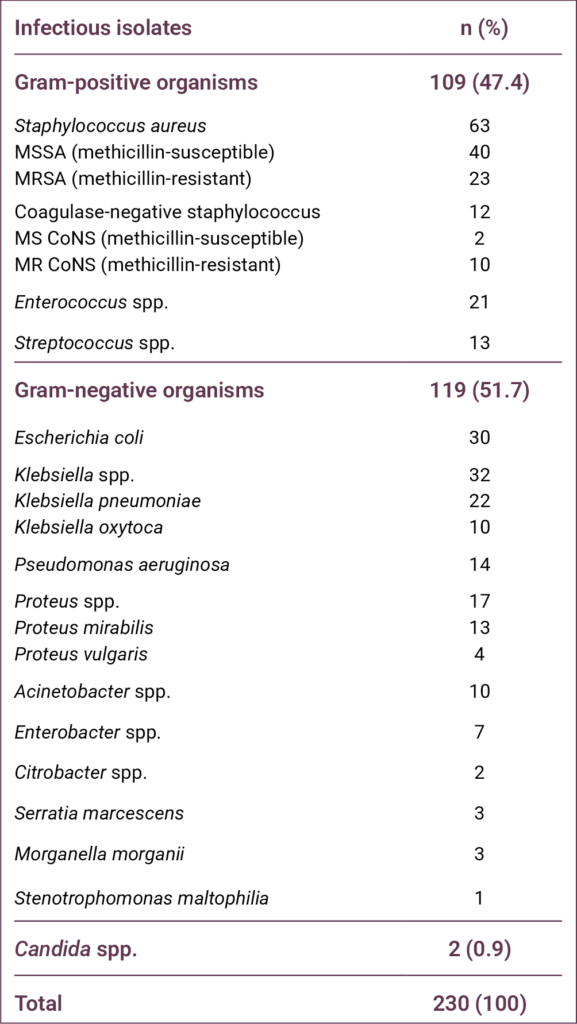
The most frequently isolated pathogen was S. aureus (n = 63, 27.4%), including 23 (10%) MRSA isolates. The second and third most common pathogens were Klebsiella spp. (n = 32, 13.9%) and Escherichia coli (n = 30, 13%), respectively.
Discussion
Studies conducted over the past several decades have demonstrated that the distribution of pathogens in patients with diabetes-related foot infections varies not only by region but also by country. When these studies are examined collectively, the world can be broadly categorized into two epidemiological regions. The first includes Europe and North America, where Gram-positive organisms predominate. The second comprises temperate regions encompassing Africa and Asia, where Gram-negative organisms are more prevalent, and the proportion of Pseudomonas aeruginosa is notably high (8). Studies conducted in Türkiye have generally indicated that the country aligns more closely with the second epidemiological pattern. For example, in a study covering a 15-year period, Gram-positive organisms accounted for 45.8% of isolates, whereas Gram-negative organisms accounted for 53.7% (9). In the same study, a statistically significant trend was observed over time, with Gram-positive pathogens increasing and Gram-negative pathogens decreasing. The distribution observed in our study was similar to these previously reported findings. Regarding specific pathogens, S. aureus, P. aeruginosa, and E. coli were consistently among the most frequently encountered organisms over the 15-year period, although their relative ranking varied by year (9). In a multicenter study by Acar et al. (10), which compared the pre–COVID-19 period with the pandemic period, a significant reduction in the number of specimens obtained for microbiological analysis during the pandemic was observed; however, no substantial change in pathogen distribution was identified. In that study, the most frequently isolated organisms were Pseudomonas spp. (16.4%) and S. aureus (15%) (10).
The findings of our study warrant particular discussion regarding P. aeruginosa. In the majority of studies conducted in Türkiye on diabetes-related foot infections, this pathogen has ranked either first or second among the most frequently isolated organisms (11–14). In contrast, in our study, P. aeruginosa ranked fifth. One important limitation of the existing literature in this field is that most studies have been conducted in tertiary-care hospitals, which may substantially influence pathogen distribution. Because our study was performed in a secondary-care state hospital, other Gram-negative organisms such as Klebsiella spp. (13.9%), E. coli (13%), and Proteus spp. (7.4%) may have become more prominent. Furthermore, Enterococcus spp. (9.1%), which has not been reported as a leading pathogen in several previous studies, was among the most frequently isolated organisms in our cohort.
Although an overall increase in Gram-positive pathogens has been observed in recent years in Türkiye, the proportion of S. aureus and, consequently, MRSA has reportedly declined. In a meta-analysis of studies conducted in Türkiye over the past two decades, the prevalence of S. aureus decreased from 29.4% to 18.1%, while the prevalence of MRSA declined from 12.5% to 5.5% (9). In that meta-analysis, the observed increase in Gram-positive organisms was primarily attributed to rising rates of Enterococcus spp. and Streptococcus spp. (9). In another recently published study presenting one-year data from five centers, the proportion of S. aureus was 14.6%, and the overall MRSA rate among all isolates was approximately 3% (15). In contrast to these reports, the proportion of S. aureus in our study was 27.4%, and the MRSA rate was 10%, both of which are considerably high. The elevated rates of S. aureus and MRSA observed in our cohort may indicate that pathogen distribution patterns in Türkiye are continuing to evolve. Nevertheless, our findings require confirmation through additional large-scale and multicenter studies.
Although relatively uncommon, fungal pathogens may also be implicated in diabetes-related foot infections, and pre-existing fungal infection of the foot or nails has been identified as a significant risk factor (16). In our study, Candida spp. was isolated from only two specimens, resulting in a very low prevalence.
The most important limitation of our study is the inability to evaluate anaerobic bacteria. Due to inadequate laboratory infrastructure, we were unable to assess the presence and distribution of anaerobic pathogens, which may represent a significant component of polymicrobial diabetes-related foot infections.
Conclusion
Our study revealed two key observations. First, the proportion of S. aureus and MRSA among patients presenting to our hospital with diabetes-related foot infections was relatively high. Second, although many studies conducted in Türkiye have reported a high prevalence of P. aeruginosa, this pathogen was not among the most frequently isolated organisms in our cohort. These results underscore the importance of local microbiological surveillance in guiding empirical antimicrobial therapy for diabetes-related foot infections. Further multicenter studies conducted in different regions are needed to confirm and expand upon these findings.
REFERENCES
Tentolouris N, Petrikkos G, Vallianou N, Zachos C, Daikos GL, Tsapogas P, et al. Prevalence of methicillin-resistant Staphylococcus aureus in infected and uninfected diabetic foot ulcers. Clin Microbiol Infect. 2006;12(2):186–9. [CrossRef]
Turhan V, Mutluoglu M, Acar A, Hatipoğlu M, Önem Y, Uzun G, et al. Increasing incidence of Gram-negative organisms in bacterial agents isolated from diabetic foot ulcers. J Infect Dev Ctries. 2013;7(10):707–12. [CrossRef]
Ndosi M, Wright-Hughes A, Brown S, Backhouse M, Lipsky BA, Bhogal M, et al. Prognosis of the infected diabetic foot ulcer: a 12-month prospective observational study. Diabet Med. 2018;35(1):78–88. [CrossRef]
Senneville E, Albalawi Z, van Asten SA, Abbas ZG, Allison G, Aragon-Sanchez J, et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab Res Rev. 2024;40(3):e3687. [CrossRef]
Mitov I, Strateva T, Markova B. Prevalence of virulence genes among Bulgarian nosocomial and cystic fibrosis isolates of Pseudomonas aeruginosa. Braz J Microbiol. 2010;41(3):588–95. [CrossRef]
Ertugrul MB. [Medical therapy in diabetic foot infection]. TOTBID Derg. 2015;14(5):404–12. Turkish.
Ertuğrul B, Uçkay I, Schöni M, Peter-Riesch B, Lipsky BA. Management of diabetic foot infections in the light of recent literature and new international guidelines. Expert Rev Anti Infect Ther. 2020;18(4):293–305. [CrossRef]
Look DC, Stoll LL, Romig SA, Humlicek A, Britigan BE, Denning GM. Pyocyanin and its precursor phenazine-1-carboxylic acid increase IL-8 and intercellular adhesion molecule-1 expression in human airway epithelial cells by oxidant-dependent mechanisms. J Immunol. 2005;175(6):4017–23. [CrossRef]
Chantelau E, Kushner T, Spraul M. How effective is cushioned therapeutic footwear in protecting diabetic feet? A clinical study. Diabet Med. 1990;7(4):355–9. [CrossRef]
Acar A, Saltoğlu N, Tülek N, Turhan Ö, Serin EN, Yapar D, et al. Impact of the COVID-19 pandemic on diabetic foot patients: a shift in the infectious agent profile toward nonfermentative Gram-negative bacilli. J Am Podiatr Med Assoc. 2024;114(3):22–073. [CrossRef]
Ertugrul BM, Oncul O, Tulek N, Willke A, Sacar S, Tunccan OG, et al. A prospective, multi-center study: factors related to the management of diabetic foot infections. Eur J Clin Microbiol Infect Dis. 2012;31(9):2345–52. [CrossRef]
Ertugrul MB, Baktiroglu S, Salman S, Unal S, Aksoy M, Berberoglu K, et al. Pathogens isolated from deep soft tissue and bone in patients with diabetic foot infections. J Am Podiatr Med Assoc. 2008;98(4):290–5. [CrossRef]
Ertuğrul MB, Uyar-Güleç G, Baktıroğlu S, Çörekli E, Türe M. [The Distribution of Causative Microorganisms in Diabetic Foot Infection: Have There Been Any Alterations? ]. Klimik Derg. 2017;30(1):27–31. Turkish. [CrossRef]
Utlu Y, Başak O, Bozkurt-Kozan F, Ertuğrul MB. [Causative agents and factors associated with multidrug-resistant pathogens in diabetic foot infections]. Klimik Derg. 2019;32(1):84–9. Turkish. [CrossRef]
Gellatly SL, Hancock RE. Pseudomonas aeruginosa: new insights into pathogenesis and host defenses. Pathog Dis. 2013; 67(3):159–73. [CrossRef]
Bristow IR, Spruce MC. Fungal foot infection, cellulitis, and diabetes: a review. Diabet Med. 2009;26(5):548–51. [CrossRef]