

Abstract
Keywords:Diabetic foot ulcer, albumin, total protein, immunonutrition
Introduction
Diabetic foot ulceration (DFU) is one of the most common and debilitating complications of diabetes mellitus (DM). The lifetime incidence of DFU in individuals with DM has been reported to be as high as 25%. Diabetic foot ulceration represents a major public health concern due to its association with impaired quality of life, high recurrence rates, increased risk of amputation, and elevated mortality (1–3).
The management of DFU is often complex and costly, frequently requiring prolonged hospitalization and multidisciplinary treatment approaches. In the United States, approximately one-third of the direct healthcare costs associated with DM and its complications are attributed to diabetic foot ulcers (4). With the global prevalence of DM increasing rapidly, the incidence of DFU is also expected to increase further in the coming years.
Effective prevention and management of DFU require careful clinical evaluation and comprehensive treatment strategies. Patient education, optimal metabolic control, identification of risk factors, and early intervention are critical components in preventing DFU progression (3). Multidisciplinary management, including medical therapy, surgical intervention, infection control, vascular assessment, and nutritional support, is recommended to improve clinical outcomes (5).
Malnutrition is recognized as an important systemic factor affecting wound healing in chronic wounds such as DFU. Adequate nutritional support may improve immune response, reduce infection risk, and promote tissue repair, particularly in older adults. Monitoring nutritional biomarkers, such as serum albumin and prealbumin, may provide valuable information on the nutritional status of patients with chronic wounds (6,7).
The present study aimed to evaluate the association between routine clinical use of an oral immunonutrition supplement and changes in serum albumin and total protein levels, as well as wound measurements in hospitalized patients with DFU.
Materials and Methods
This study was designed as a prospective cohort study conducted between May 2023 and October 2023 at the Diabetic Foot Service of Hitit University Erol Olçok Training and Research Hospital. Adult patients hospitalized with a diagnosis of DFU who agreed to participate in the study were included. Ethical approval for the study was obtained from the Hitit University Faculty of Medicine Clinical Research Ethics Committee on March 29, 2023, with decision no. 2023-44.
Within the routine clinical nutritional support protocol of the service, some patients received an oral immunonutrition supplement containing arginine, omega-3 fatty acids, and RNA based on their clinical condition and laboratory findings. Each 237 mL serving of the supplement contained 18 g of protein, 4.3 g arginine, 1.4 g omega-3 fatty acids, and 0.43 g RNA.
Patients with normal renal function parameters (urea and creatinine levels) received the supplement twice daily for 30 days as part of routine clinical care. Patients with elevated renal function parameters did not receive immunonutrition supplementation. Accordingly, patients were categorized into two cohorts: those receiving oral immunonutrition and those not receiving it.
Diabetic foot ulcers were classified according to the Wagner classification system. Daily dietary intake records were collected for 15 days, and average daily protein intake was calculated using the Turkish National Food Composition Database. Clinical data, including serum albumin, total protein, and creatinine levels, were obtained from the hospital information system. Ulcer measurements were performed at baseline and on day 30 using a sterile disposable ruler. No modifications were made to systemic or local treatment protocols routinely applied in the diabetic foot unit during the study period.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro-Wilk test. Continuous variables were compared using the independent samples t test or the Mann-Whitney U test, depending on the distribution. Categorical variables were compared using the Pearson’s chi-square test or Fisher’s exact test when appropriate. Multivariate linear regression analysis was conducted to evaluate the association between immunonutrition supplementation and changes in serum albumin, total protein levels, and wound size, while accounting for potential confounding variables, including renal function parameters. A p-value < 0.05 was considered statistically significant.
Results
A total of 72 patients hospitalized with diabetic foot ulcers were included in the study and divided into the intervention group (n = 36) and the control group (n = 36). Among these patients, 36.9% (n = 24) were female, and the mean age was 65.1 ± 9.2 years. The mean daily dietary protein intake was 95 ± 5.9 g/day.
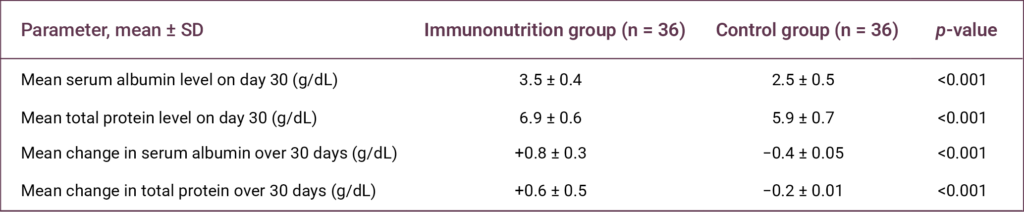
A statistically significant association was observed between the use of the oral immunonutrition supplementation and both serum albumin and total protein levels on day 30, as well as changes in these parameters during the 30-day follow-up period (p < 0.001 for all comparisons) (Table 1).
On day 30, the mean serum albumin and total protein levels in the intervention group were 3.5 ± 0.4 g/dL and 6.9 ± 0.6 g/dL, respectively. In contrast, the control group had mean levels of 2.5 ± 0.5 g/dL and 5.9 ± 0.7 g/dL, respectively (Table 1).
During the 30-day follow-up period, serum albumin and total protein levels increased by 0.8 ± 0.3 g/dL and 0.6 ± 0.5 g/dL, respectively, in the intervention group. In the control group, these parameters decreased by 0.4 ± 0.05 g/dL and 0.2 ± 0.01 g/dL, respectively (Table 1).

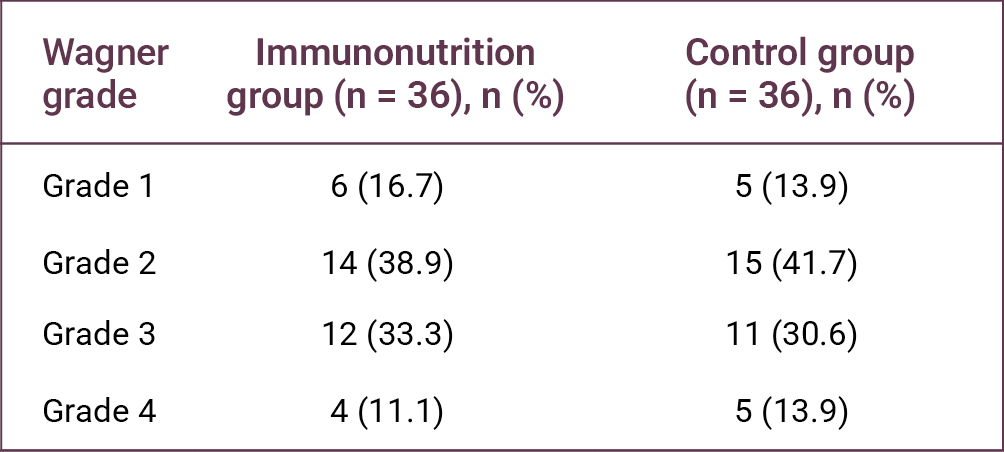
No statistically significant difference was observed between the Wagner ulcer stages of the two groups (p > 0.05) (Table 2). However, a statistically significant difference was found in ulcer length reduction between the groups (p = 0.008) (Table 3).
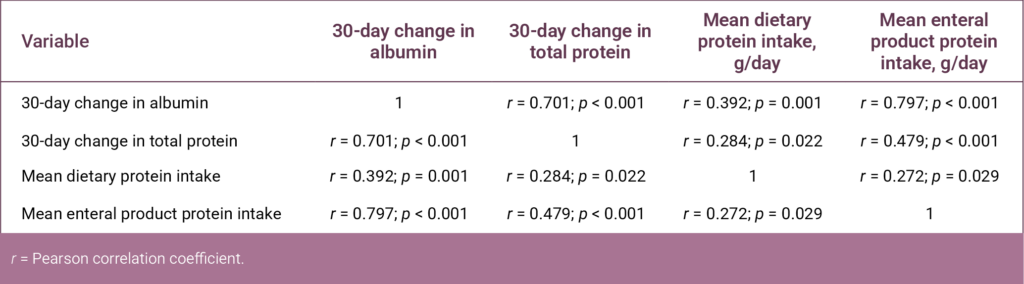
Correlation analysis revealed significant correlations between changes in serum albumin and total protein levels and dietary protein intake variables (Table 4).
Discussion
With the global increase in DM cases, inadequate long-term glycemic control in patients with DM causes damage to the distal microvasculature and eventually leads to the development of diabetic foot ulcers (8). Diabetic foot ulcers are one of the most important chronic complications in patients with DM, often requiring surgical intervention and imposing substantial morbidity and economic burden on patients (9).
Systemic factors play an important role in the wound-healing process in the management of chronic wounds. Diabetic foot ulcers generally begin with minor injuries that go unnoticed due to diabetic neuropathy, and the combination of immunological, vascular, nutritional, glycemic, and infectious factors may affect wound healing (9).
In this study, the association between routine immunonutrition support administered as part of routine clinical practice in our hospital and changes in serum albumin and total protein levels, as well as wound measurements, in patients with DFU was evaluated. The findings demonstrated a statistically significant association between changes in serum albumin and total protein levels and the reduction in ulcer length in patients receiving oral immunonutrition support.
Several studies have reported an inverse relationship between serum albumin level, an important indicator of nutritional status, and the risk of amputation in patients with DFU (10–12). It has also been stated that a decrease in albumin level may not only reflect nutritional status but may also be associated with the clinical severity of the disease, including infectious and inflammatory processes (13).
In conclusion, oral immunonutrition supplementation in hospitalized patients with DFU was associated with increased serum albumin and total protein levels. In addition, a significant association was observed between oral immunonutrition supplementation and a reduction in ulcer length during the follow-up period. However, no statistically significant difference was found in ulcer stage between the two groups. Larger prospective studies with longer follow-up periods are needed to further clarify the potential effects of immunonutrition support on wound healing in patients with DFU.
REFERENCES
Vileikyte L. Psychosocial and behavioral aspects of diabetic foot lesions. Curr Diab Rep. 2008;8(2):119–25. [CrossRef]
Dubský M, Jirkovská A, Bem R, Fejfarová V, Skibová J, Schaper NC, et al. Risk factors for recurrence of diabetic foot ulcers: prospective follow-up analysis in the Eurodiale subgroup. Int Wound J. 2013;10(5):555–61. [CrossRef]
Brownrigg JR, Davey J, Holt PJ, Davis WA, Thompson MM, Ray KK, et al. The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis. Diabetologia. 2012;55(11):2906–12. [CrossRef]
Driver VR, Fabbi M, Lavery LA, Gibbons G. The costs of diabetic foot: the economic case for the limb salvage team. J Vasc Surg. 2010;52(3 Suppl):17S–22S. Erratum in: J Vasc Surg. 2010;52(6):1751. [CrossRef]
Blume P, Wu S. Updating the diabetic foot treatment algorithm: recommendations on treatment using advanced medicine and therapies. Wounds. 2018;30(2):29–35.
Maier HM, Ilich JZ, Kim JS, Spicer MT. Nutrition supplementation for diabetic wound healing: a systematic review of current literature. Skinmed. 2013;11(4):217–24; quiz 224–5.
Arnold M, Barbul A. Nutrition and wound healing. Plast Reconstr Surg. 2006;117(7 Suppl):42S–58S. [CrossRef]
Chinese Diabetes Society, Society of Infectious Disease, Chinese Medical Association of Organization Repair and Regeneration Branch. [Chinese Guidelines for the Prevention and Treatment of Diabetic Foot (2019 edition)]. Chin J Diabetes. 2019;11:92–108. Chinese.
Shakil S, Khan AU. Infected foot ulcers in male and female diabetic patients: a clinico-bioinformative study. Ann Clin Microbiol Antimicrob. 2010;9:2. [CrossRef]
Yusof NM, Rahman JA, Zulkifly AH, Che-Ahmad A, Khalid KA, Sulong AF, et al. Predictors of major lower limb amputation among type II diabetic patients admitted for diabetic foot problems. Singapore Med J. 2015;56(11):626–31. [CrossRef]
Leung HB, Ho YC, Carnett J, Lam PK, Wong WC. Diabetic foot ulcers in the Hong Kong Chinese population: retrospective study. Hong Kong Med J. 2001;7(4):350–5.
Akinci B, Yener S, Yesil S, Yapar N, Kucukyavas Y, Bayraktar F. Acute phase reactants predict the risk of amputation in diabetic foot infection. J Am Podiatr Med Assoc. 2011;101(1):1–6. [CrossRef]
Xu S, Wang Y, Hu Z, Ma L, Zhang F, Liu P. Effects of neutrophil-tolymphocyte ratio, serum calcium, and serum albumin on prognosis in patients with diabetic foot. Int Wound J. 2023;20:1638–46.