Abstract
Keywords: Family medicine, chronic wound, wound care, debridement, dressing materials
Introduction
Chronic wound healing, regardless of etiological origin, is a complex pathological process in which normal wound-healing stages fail to be completed within the expected timeframe, and such wounds are often prone to infection and biofilm formation (1). This condition, increasingly recognized as a global health concern, affects approximately 40 million people and, despite advances in modern medical technologies, imposes a difficult-to-sustain economic burden on healthcare systems due to its treatment-resistant nature. In particular, the rapidly increasing aging population, together with accompanying comorbidities such as diabetes and hypertension and broader demographic changes, is driving the prevalence of chronic wounds toward what has been described as a "silent pandemic" (2).
Chronic wounds are defined as wounds that do not follow the normal healing process and generally fail to heal within four to six weeks (3). These wounds often remain in the inflammatory phase (4). It is estimated that 1–2% of the global population will experience a chronic wound during their lifetime (5). Factors such as diabetes, venous hypertension, peripheral artery disease, poor nutrition, wound bed hypoxia, and infection contribute to the chronicity of wounds (6). While the normal healing process consists of hemostasis, inflammation, proliferation, and maturation phases, this balance is disrupted in chronic wounds (7). In chronic wound management, debridement of necrotic tissue, infection control, maintenance of appropriate moisture balance, and pressure relief are fundamental steps (8). Treatment may involve modern dressing materials, such as hydrocolloids, alginates, and hydrogels, or advanced methods, such as negative-pressure wound therapy, depending on the wound characteristics. One of the key factors exacerbating the problem is the reduction of chronic wound management to simple wound dressing and the lack of a multidisciplinary approach. Although primary healthcare services represent a strategic component in managing this problem, the competence of family physicians in current debridement techniques, wound-bed preparation (TIME [Tissue, Infection/Inflammation, Moisture, Edge] and TIMERS [Tissue, Infection/Inflammation, Moisture, Edge, Repair/Regeneration, Social factors] frameworks), and modern dressing materials remains a subject of debate. Nonstandardized diagnosis and treatment approaches may result in prolonged healing times, costly complications, and deterioration in patients' quality of life.
Primary healthcare services play a critical role in the early diagnosis, treatment, and patient education processes of chronic wounds. Improving family physicians' knowledge in this area may enhance patient outcomes and help reduce the burden on the healthcare system (9).
This study aimed to evaluate the knowledge levels and clinical approaches of family physicians regarding chronic wound care, including debridement management, infection control, and current dressing materials.
Materials and Methods
The population of this descriptive study consisted of 470 contracted family physicians working in Manisa province, Türkiye. During the research process, we aimed to recruit as many family physicians as possible who agreed to participate in the study within the specified dates.
Some of the family physicians declined to participate, and the research was completed with the participation of family physicians who volunteered for the study. The overall participation rate was 86.2%. The study protocol was approved by the Manisa Celal Bayar University Faculty of Medicine Health Sciences Ethics Committee on September 6, 2023 (No: 20.478.486/987).
Data were collected using a 93-item knowledge questionnaire. The first section included questions on the demographic and occupational characteristics of the participants, and the second section covered the knowledge of chronic wound management, including the TIMERS framework, general wound care, dressing, and wound types (diabetic, venous, ischemic, and pressure ulcers).
In evaluating the knowledge questionnaire, 1 point was awarded for each correct response, and 0 points were assigned for incorrect or unanswered items. The raw scores were converted to a 100-point scale (number of correct responses / total number of questions × 100) and standardized as the "knowledge success score" to facilitate comparative analysis. Data were collected after obtaining written informed consent from the participants.
Data were analyzed using IBM SPSS Statistics version 27.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were expressed as numbers (n), percentages (%), means ± standard deviations (SD), and medians (minimum–maximum). The normality of numerical data was assessed using the Shapiro-Wilk test.
For comparisons between two groups, the independent samples t-test was used when the data were normally distributed, and the Mann-Whitney U test was used when they were not. Cronbach’s α coefficients were calculated to assess scale reliability and internal consistency. The competency levels and knowledge gaps of physicians in chronic wound management were visualized using a radar chart (spider chart). A p-value < 0.05 was considered statistically significant.
Results
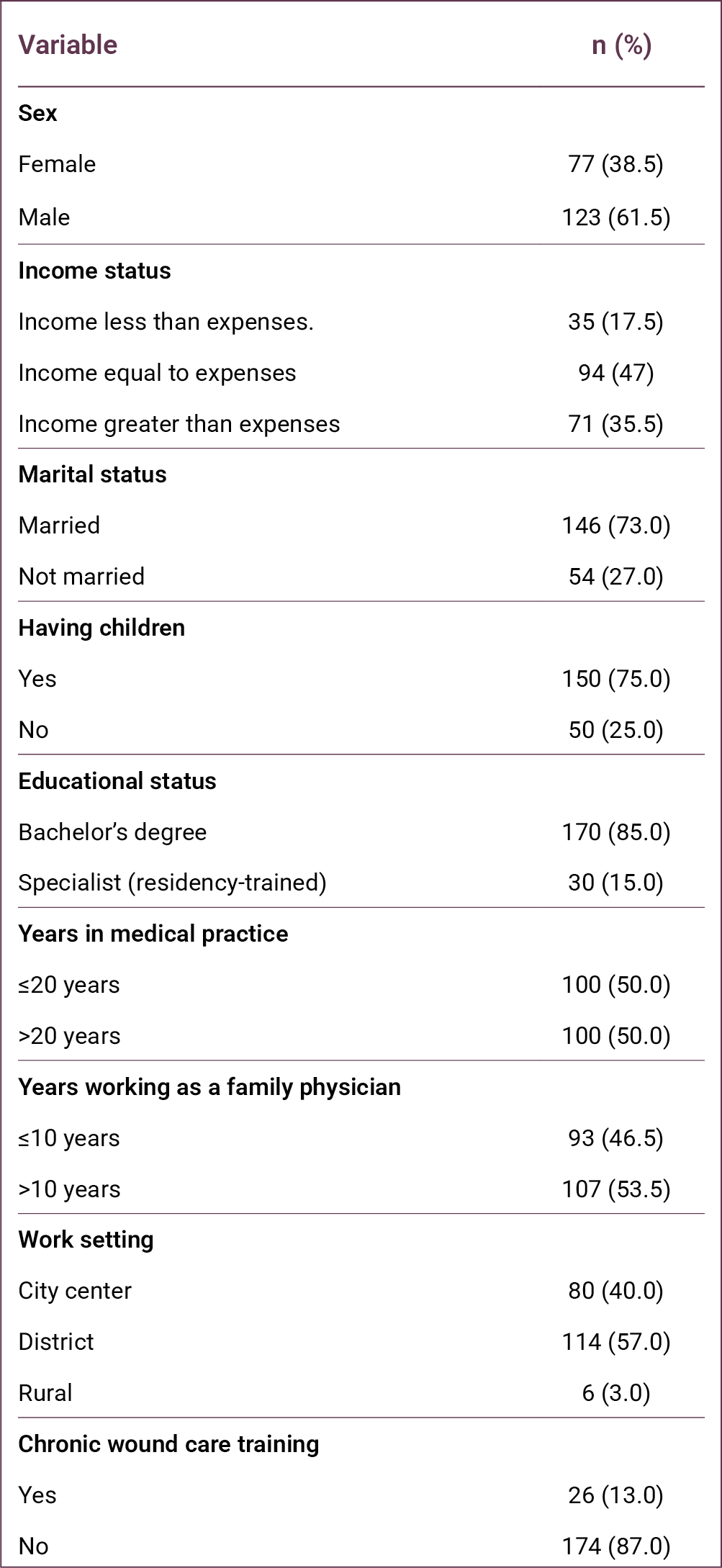
The study was conducted with 200 family physicians among the 470 working in Manisa province. Of the participants, 123 (61.5%) were male, 146 (73%) were married, 150 (75%) had children, and 156 (78%) lived with their spouse or children. Regarding economic status, 94 (47%) reported that their income was equal to their expenses. In terms of professional status, 157 (78.5%) were general practitioners, 13 (6.5%) were family medicine residents working under contract, and 30 (15%) were family medicine specialists. Only 26 (13%) physicians had received training in wound care (Table 1).
Women physicians had a higher mean number of correct responses (61.25 ± 18.41) compared with male physicians (56.93 ± 21.26). Physicians with a bachelor's degree answered 57.81 ± 20.32 questions correctly, whereas those with specialist training answered 63.03 ± 19.73 questions correctly. Physicians working in the city center answered 56.56 ± 20.40 questions correctly, while those working in districts and rural areas answered 59.95 ± 20.16 questions correctly.
When years of professional experience were examined, physicians with ≤20 years of experience answered 59.31 ± 20.04 questions correctly, while those with >20 years of experience answered 57.89 ± 20.57 questions correctly. Similarly, based on years of experience in family medicine, physicians with ≤10 years of experience answered 57.87 ± 21.66 questions correctly, while those with >10 years of experience answered 59.23 ± 19.07 questions correctly.
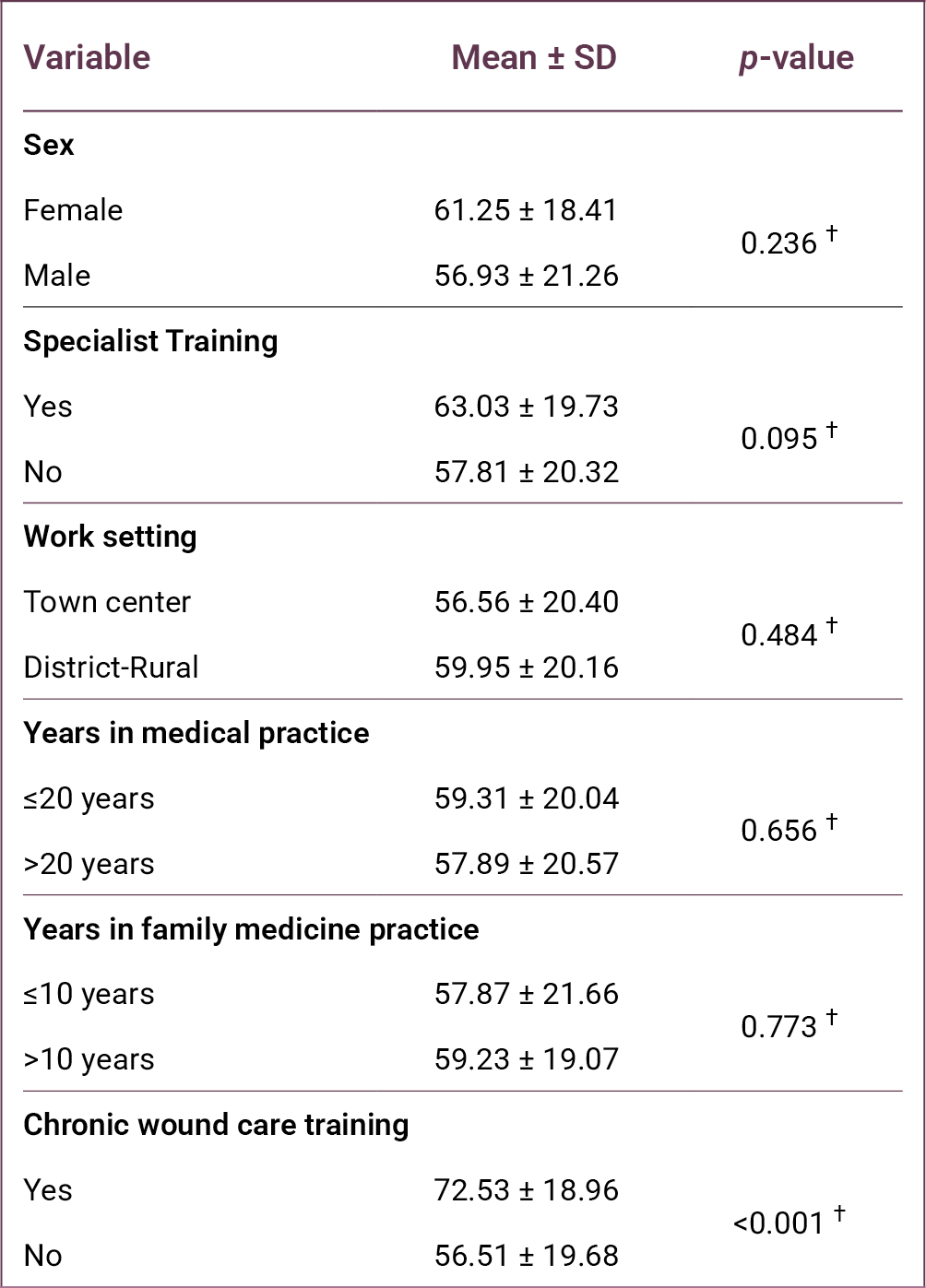
Among all variables examined, only the difference associated with wound care training was statistically significant (p < 0.001). Physicians who had received chronic wound care training answered 72.53 ± 18.96 questions correctly, whereas those without such training answered 56.51 ± 19.68 questions correctly.
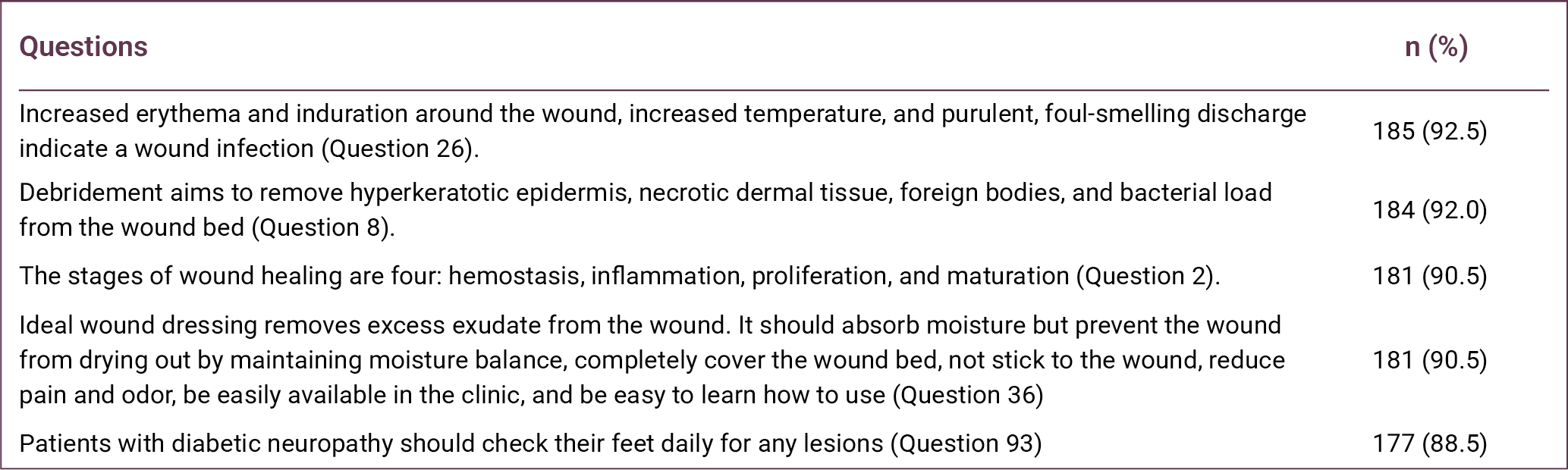
Question 26, regarding indicators of wound infection, had the highest number of correct responses (n = 185). This was followed by Question 8, which assessed knowledge of the purpose of debridement (n = 184). Question 2, related to the stages of wound healing, ranked third with 181 correct responses (Table 3).
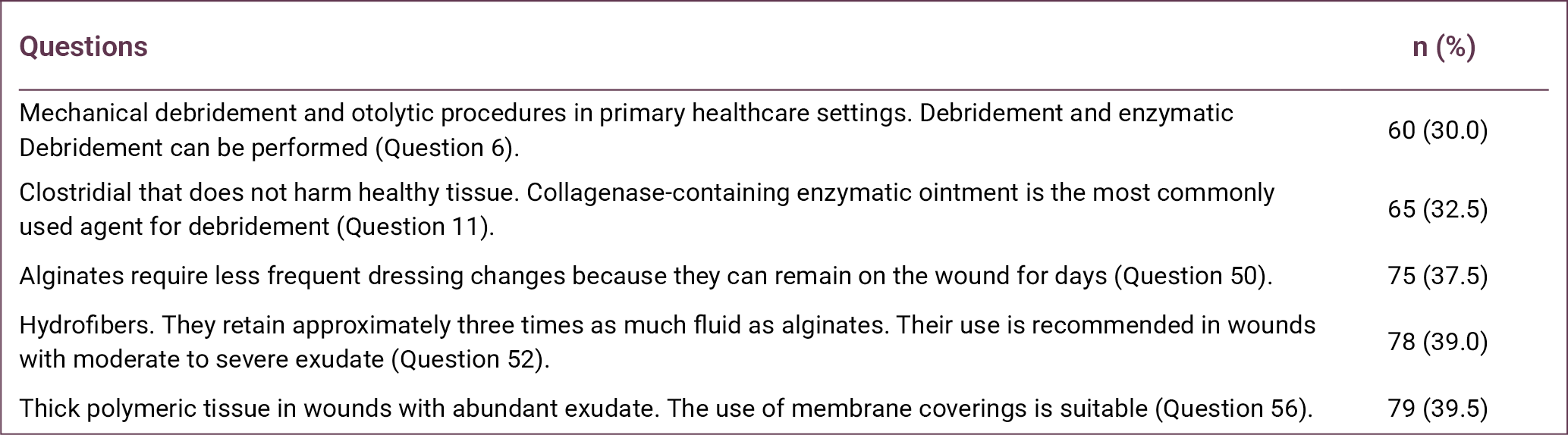
In contrast, Question 6, which addressed the types of debridement that can be performed in primary healthcare settings, had the lowest number of correct responses (n = 60). Question 11, concerning the most commonly used agent for enzymatic debridement, had the second lowest number of correct responses (n = 65). Question 50, regarding the replacement period of alginates, ranked third lowest with 75 correct responses (Table 4).
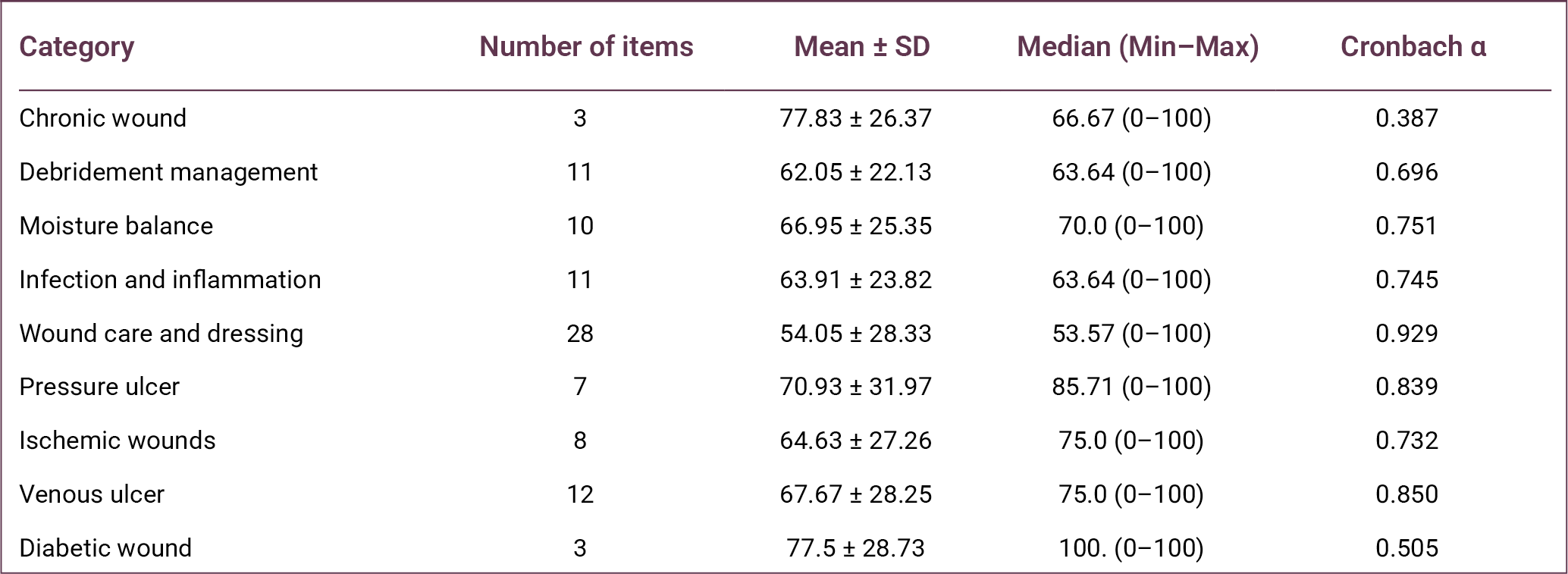
Reliability analyses of the subdimensions of the knowledge questionnaire used in the study are presented in Table 5. Cronbach’s α coefficients demonstrated high reliability for the subdimensions of wound care and dressing (0.929), venous wounds (0.850), and pressure ulcers (0.839). Acceptable reliability was observed for moisture balance (0.751), infection and inflammation (0.745), ischemic wounds (0.732), and debridement management (0.696).
Lower reliability values were observed for the chronic wound (0.387) and diabetic wound (0.505) subdimensions, likely due to the limited number of items in these categories. When the knowledge categories were examined, family physicians achieved the highest success rate in the chronic wound category (77.83%), whereas the lowest success rate was observed in the wound care and dressing category (54.05%).
The radar (spider) chart presented in Figure 1 illustrates the distribution of family physicians’ competencies and knowledge gaps in chronic wound management. The chart demonstrates an asymmetrical distribution of knowledge across categories. The chronic wound category is positioned closest to the outer edge of the chart, indicating the highest level of knowledge. Conversely, the wound care and dressing category lies closest to the center, indicating the lowest level of performance.
The relationship between receiving chronic wound care training and knowledge scores is presented in Table 6. Physicians who had received training (n = 26) demonstrated significantly higher scores than those without training (n = 174) across nearly all categories.
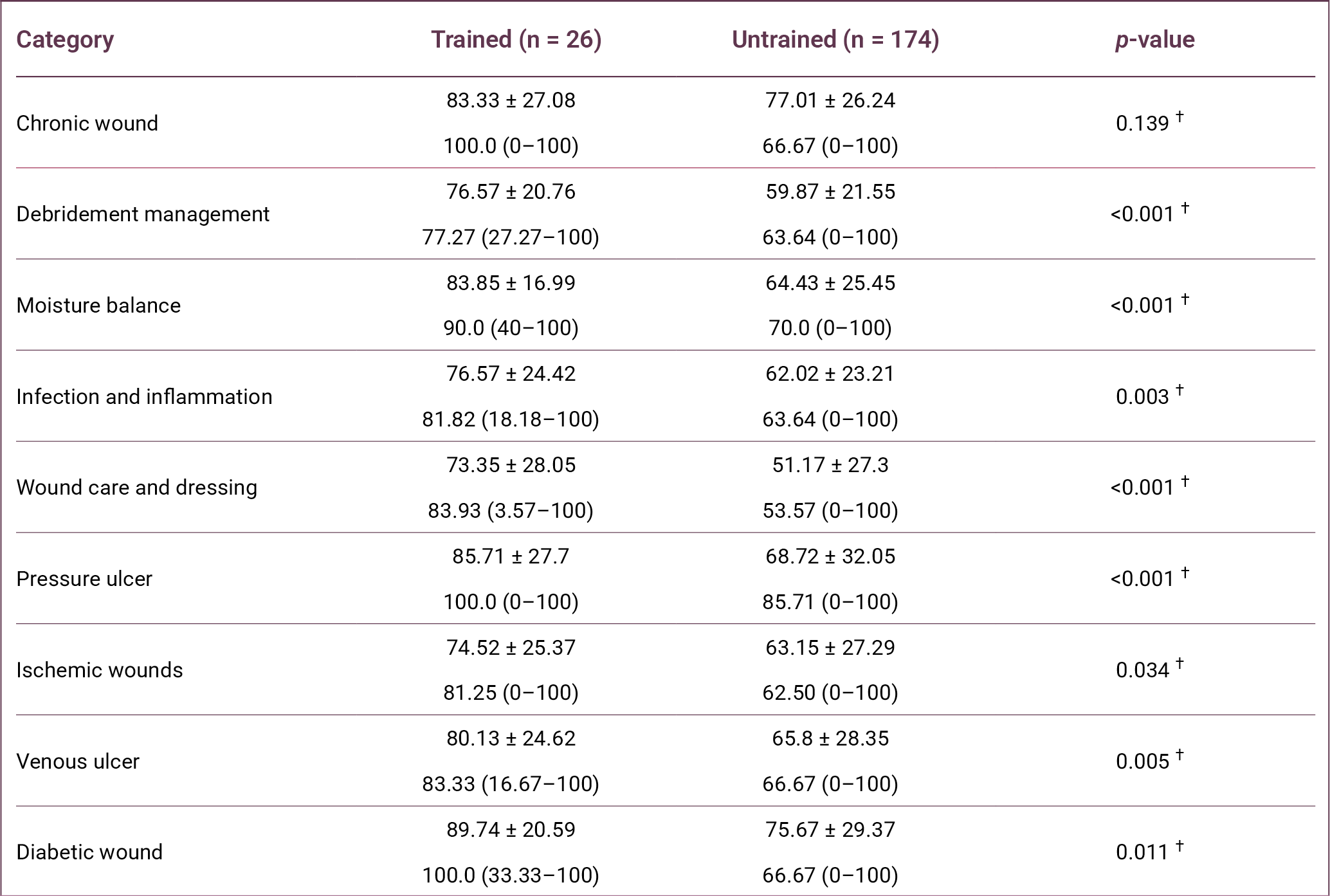
In the debridement management category, the success rate was 76.57% in the trained group and 59.87% in the untrained group (p < 0.001). In the moisture balance category, success rates were 83.85% in the trained group and 64.43% in the untrained group (p < 0.001).
In the wound care and dressing category, which showed the lowest overall success rate, the trained group achieved 73.35%, whereas the untrained group achieved 51.17% (p < 0.001). In the pressure ulcer category, the success rate in the trained group (85.71%) was also significantly higher than in the untrained group (68.72%) (p < 0.001).
Similarly, in the infection and inflammation category, physicians who received training scored significantly higher (76.57%) than those without training (62.02%) (p = 0.003). In the vascular and diabetic wound categories, trained physicians also demonstrated significantly higher knowledge levels in venous wounds (p = 0.005), ischemic wounds (p = 0.034), and diabetic wounds (p = 0.011).
However, in the chronic wound definition category, the difference between the trained group (83.33%) and the untrained group (77.01%) was not statistically significant (p = 0.139).
Discussion
This study evaluated the competencies and clinical approaches of family physicians, who play a central role in primary healthcare services, in chronic wound care, debridement management, infection control, and the use of current dressing materials. The findings indicate that family physicians demonstrate a high level of awareness regarding the recognition and the general definition of chronic wounds, but substantial knowledge gaps remain in practical management and technical interventions.
Chronic wounds represent a major clinical and economic burden for healthcare systems and significantly impair patients' quality of life. Since no single medical specialty is responsible for the management of chronic wounds, their care requires a multidisciplinary approach involving multiple levels of the healthcare system.
Family medicine is a comprehensive medical specialty that provides continuous, person-centered care across all age groups and health conditions, integrating clinical and behavioral sciences while remaining easily accessible within the community (10). Within this framework, family physicians often represent the first point of contact for patients presenting with chronic wounds, placing them in a key position for early assessment and initial management. Therefore, strengthening wound care competencies in primary care is essential and necessitates the development of structured training programs.
Adequate wound care training enables physicians to perform appropriate wound assessment, initiate evidence-based treatment, and identify cases requiring referral to specialized care. Timely and effective wound management at the primary care level may reduce unnecessary referrals to secondary and tertiary healthcare services while improving patient outcomes.
In this study, the knowledge levels of family physicians regarding chronic wound management were examined, and the significant impact of training status on knowledge and competency levels was demonstrated. The finding that only 13% of participants had received wound care training highlights a substantial educational gap in primary healthcare settings.
Consistent with our findings, the study by Şahan et al. (11) reported that only 19 (10.67%) participants had received wound care training within the previous four years. In the present study, wound care training was associated with significantly higher knowledge scores, particularly in areas requiring technical competence such as debridement management (p < 0.001), moisture balance (p < 0.001), and wound care and dressing practices (p < 0.001).
Similarly, the study by Fernández-Araque et al. (12) demonstrated that greater exposure to wound care training was associated with improved knowledge levels. Şahan et al. (11) also reported a statistically significant relationship between wound care training and knowledge test performance.
The finding that physicians without training achieved only a 51.17% success rate in the dressing materials category suggests that modern wound management approaches, such as hydrocolloids and silver-containing dressings, may not be sufficiently integrated into routine clinical practice (11).
This study has several limitations. First, it was conducted among family physicians working in a single province, and therefore, the findings may not be generalizable to all primary care physicians in Türkiye. Second, data were collected using a self-report questionnaire that primarily reflects participants' theoretical knowledge rather than their clinical practice. Finally, the cross-sectional study design prevents the establishment of causal relationships between the variables examined.
In conclusion, effective chronic wound management in primary healthcare requires not only the ability to recognize and classify wounds but also sufficient knowledge of modern wound care interventions and dressing materials. The findings of this study indicate that important knowledge gaps persist in the practical management of chronic wounds among family physicians. Expanding wound care training programs and integrating structured wound management education into undergraduate medical curricula and family medicine residency training may help strengthen physicians’ competencies and improve the quality of chronic wound care in primary healthcare settings.
REFERENCES
Öztaş P. [Wound healing, care, and treatment]. Ankara Eğt Arş Hast Derg. 2021;54(2):341–51. Turkish. [CrossRef]
Las Heras K, Igartua M, Santos-Vizcaino E, Hernandez RM. Chronic wounds: Current status, available strategies and emerging therapeutic solutions. J Control Release. 2020;328:532–50. [CrossRef]
Graves N, Phillips CJ, Harding K. A narrative review of the epidemiology and economics of chronic wounds. Br J Dermatol. 2022;187(2):141–8. [CrossRef]
Raziyeva K, Kim Y, Zharkinbekov Z, Kassymbek K, Jimi S, Saparov A. Immunology of acute and chronic wound healing. Biomolecules. 2021;11(5):700. [CrossRef]
Sen CK. Human wound and its burden: updated 2020 compendium of estimates. Adv Wound Care (New Rochelle). 2021;10(5):281–92. [CrossRef]
Eriksson E, Liu PY, Schultz GS, Martins-Green MM, Tanaka R, Weir D, et al. Chronic wounds: Treatment consensus. Wound Repair Regen. 2022;30(2):156–71. Erratum in: Wound Repair Regen. 2022;30(4):536. [CrossRef]
Verdolino DV, Thomason HA, Fotticchia A, Cartmell S. Wound dressings: curbing inflammation in chronic wound healing. Emerg Top Life Sci. 2021;5(4):523–37. [CrossRef]
Mongkornwong A, Wongwiwat W, Chansanti O, Sukprasert P, Akaranuchat N. Hard-to-heal wounds. PSU Medical Journal, 2024;1-12.
Akman M. [The strength of primary care in Türkiye]. Türk Aile Hek Derg. 2014;18(2):70–8. Turkish.
Edwards D, Black AT, Spielfogel WD. A multidisciplinary approach to managing ischemic wounds and current treatment options. Curr Treat Options Cardio Med. 2021;23(7):51. [CrossRef]
Şahan S and Harputlu D. [Determining the knowledge levels of primary healthcare workers regarding chronic wound care]. Etkili Hemşirelik Derg. 2025;18(2): 250–61. Turkish. [CrossRef]
Fernández-Araque A, Martinez-Delgado M, Jiménez JM, López M, Castro MJ, Gila EC. Assessment of nurses' level of knowledge of the management of chronic wounds. Nurse Educ Today. 2024;134:106084. [CrossRef]
Abstract
Keywords:Diabetic foot ulcer, albumin, total protein, immunonutrition
Introduction
Diabetic foot ulceration (DFU) is one of the most common and debilitating complications of diabetes mellitus (DM). The lifetime incidence of DFU in individuals with DM has been reported to be as high as 25%. Diabetic foot ulceration represents a major public health concern due to its association with impaired quality of life, high recurrence rates, increased risk of amputation, and elevated mortality (1–3).
The management of DFU is often complex and costly, frequently requiring prolonged hospitalization and multidisciplinary treatment approaches. In the United States, approximately one-third of the direct healthcare costs associated with DM and its complications are attributed to diabetic foot ulcers (4). With the global prevalence of DM increasing rapidly, the incidence of DFU is also expected to increase further in the coming years.
Effective prevention and management of DFU require careful clinical evaluation and comprehensive treatment strategies. Patient education, optimal metabolic control, identification of risk factors, and early intervention are critical components in preventing DFU progression (3). Multidisciplinary management, including medical therapy, surgical intervention, infection control, vascular assessment, and nutritional support, is recommended to improve clinical outcomes (5).
Malnutrition is recognized as an important systemic factor affecting wound healing in chronic wounds such as DFU. Adequate nutritional support may improve immune response, reduce infection risk, and promote tissue repair, particularly in older adults. Monitoring nutritional biomarkers, such as serum albumin and prealbumin, may provide valuable information on the nutritional status of patients with chronic wounds (6,7).
The present study aimed to evaluate the association between routine clinical use of an oral immunonutrition supplement and changes in serum albumin and total protein levels, as well as wound measurements in hospitalized patients with DFU.
Materials and Methods
This study was designed as a prospective cohort study conducted between May 2023 and October 2023 at the Diabetic Foot Service of Hitit University Erol Olçok Training and Research Hospital. Adult patients hospitalized with a diagnosis of DFU who agreed to participate in the study were included. Ethical approval for the study was obtained from the Hitit University Faculty of Medicine Clinical Research Ethics Committee on March 29, 2023, with decision no. 2023-44.
Within the routine clinical nutritional support protocol of the service, some patients received an oral immunonutrition supplement containing arginine, omega-3 fatty acids, and RNA based on their clinical condition and laboratory findings. Each 237 mL serving of the supplement contained 18 g of protein, 4.3 g arginine, 1.4 g omega-3 fatty acids, and 0.43 g RNA.
Patients with normal renal function parameters (urea and creatinine levels) received the supplement twice daily for 30 days as part of routine clinical care. Patients with elevated renal function parameters did not receive immunonutrition supplementation. Accordingly, patients were categorized into two cohorts: those receiving oral immunonutrition and those not receiving it.
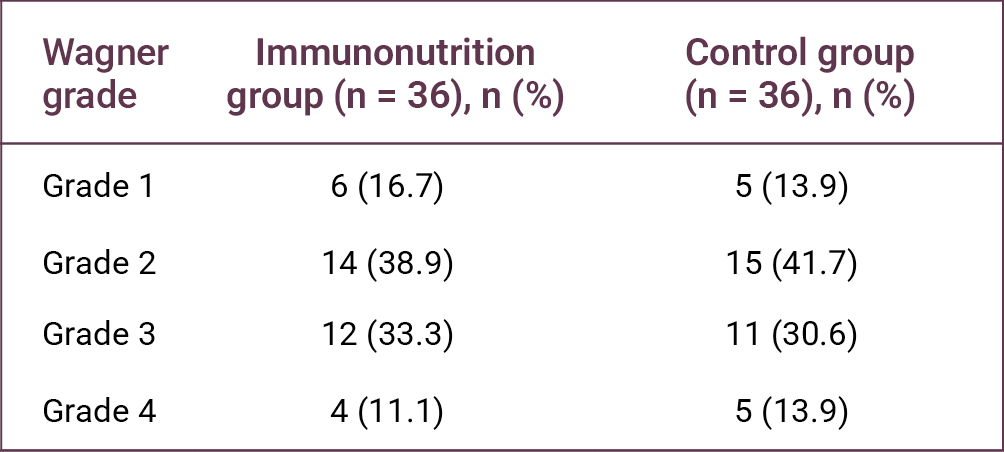
Diabetic foot ulcers were classified according to the Wagner classification system. Daily dietary intake records were collected for 15 days, and average daily protein intake was calculated using the Turkish National Food Composition Database. Clinical data, including serum albumin, total protein, and creatinine levels, were obtained from the hospital information system. Ulcer measurements were performed at baseline and on day 30 using a sterile disposable ruler. No modifications were made to systemic or local treatment protocols routinely applied in the diabetic foot unit during the study period.
Statistical analyses were performed using IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro-Wilk test. Continuous variables were compared using the independent samples t test or the Mann-Whitney U test, depending on the distribution. Categorical variables were compared using the Pearson’s chi-square test or Fisher’s exact test when appropriate. Multivariate linear regression analysis was conducted to evaluate the association between immunonutrition supplementation and changes in serum albumin, total protein levels, and wound size, while accounting for potential confounding variables, including renal function parameters. A p-value < 0.05 was considered statistically significant.
Results
A total of 72 patients hospitalized with diabetic foot ulcers were included in the study and divided into the intervention group (n = 36) and the control group (n = 36). Among these patients, 36.9% (n = 24) were female, and the mean age was 65.1 ± 9.2 years. The mean daily dietary protein intake was 95 ± 5.9 g/day.
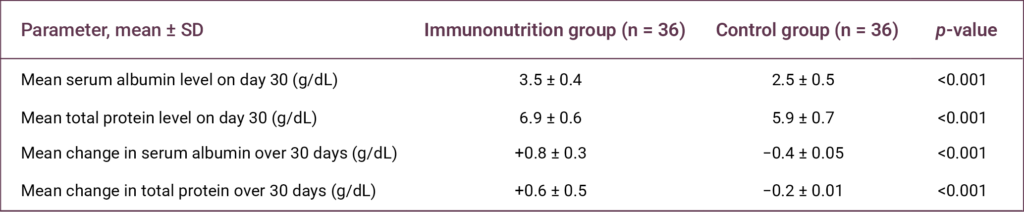
A statistically significant association was observed between the use of the oral immunonutrition supplementation and both serum albumin and total protein levels on day 30, as well as changes in these parameters during the 30-day follow-up period (p < 0.001 for all comparisons) (Table 1).
On day 30, the mean serum albumin and total protein levels in the intervention group were 3.5 ± 0.4 g/dL and 6.9 ± 0.6 g/dL, respectively. In contrast, the control group had mean levels of 2.5 ± 0.5 g/dL and 5.9 ± 0.7 g/dL, respectively (Table 1).
During the 30-day follow-up period, serum albumin and total protein levels increased by 0.8 ± 0.3 g/dL and 0.6 ± 0.5 g/dL, respectively, in the intervention group. In the control group, these parameters decreased by 0.4 ± 0.05 g/dL and 0.2 ± 0.01 g/dL, respectively (Table 1).

No statistically significant difference was observed between the Wagner ulcer stages of the two groups (p > 0.05) (Table 2). However, a statistically significant difference was found in ulcer length reduction between the groups (p = 0.008) (Table 3).
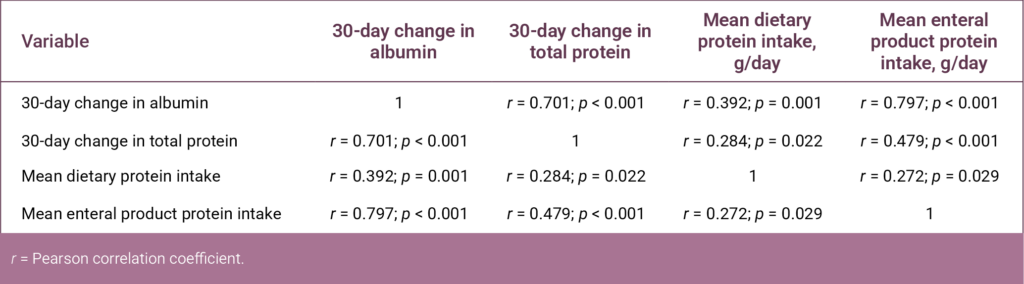
Correlation analysis revealed significant correlations between changes in serum albumin and total protein levels and dietary protein intake variables (Table 4).
Discussion
With the global increase in DM cases, inadequate long-term glycemic control in patients with DM causes damage to the distal microvasculature and eventually leads to the development of diabetic foot ulcers (8). Diabetic foot ulcers are one of the most important chronic complications in patients with DM, often requiring surgical intervention and imposing substantial morbidity and economic burden on patients (9).
Systemic factors play an important role in the wound-healing process in the management of chronic wounds. Diabetic foot ulcers generally begin with minor injuries that go unnoticed due to diabetic neuropathy, and the combination of immunological, vascular, nutritional, glycemic, and infectious factors may affect wound healing (9).
In this study, the association between routine immunonutrition support administered as part of routine clinical practice in our hospital and changes in serum albumin and total protein levels, as well as wound measurements, in patients with DFU was evaluated. The findings demonstrated a statistically significant association between changes in serum albumin and total protein levels and the reduction in ulcer length in patients receiving oral immunonutrition support.
Several studies have reported an inverse relationship between serum albumin level, an important indicator of nutritional status, and the risk of amputation in patients with DFU (10–12). It has also been stated that a decrease in albumin level may not only reflect nutritional status but may also be associated with the clinical severity of the disease, including infectious and inflammatory processes (13).
In conclusion, oral immunonutrition supplementation in hospitalized patients with DFU was associated with increased serum albumin and total protein levels. In addition, a significant association was observed between oral immunonutrition supplementation and a reduction in ulcer length during the follow-up period. However, no statistically significant difference was found in ulcer stage between the two groups. Larger prospective studies with longer follow-up periods are needed to further clarify the potential effects of immunonutrition support on wound healing in patients with DFU.
REFERENCES
Vileikyte L. Psychosocial and behavioral aspects of diabetic foot lesions. Curr Diab Rep. 2008;8(2):119–25. [CrossRef]
Dubský M, Jirkovská A, Bem R, Fejfarová V, Skibová J, Schaper NC, et al. Risk factors for recurrence of diabetic foot ulcers: prospective follow-up analysis in the Eurodiale subgroup. Int Wound J. 2013;10(5):555–61. [CrossRef]
Brownrigg JR, Davey J, Holt PJ, Davis WA, Thompson MM, Ray KK, et al. The association of ulceration of the foot with cardiovascular and all-cause mortality in patients with diabetes: a meta-analysis. Diabetologia. 2012;55(11):2906–12. [CrossRef]
Driver VR, Fabbi M, Lavery LA, Gibbons G. The costs of diabetic foot: the economic case for the limb salvage team. J Vasc Surg. 2010;52(3 Suppl):17S–22S. Erratum in: J Vasc Surg. 2010;52(6):1751. [CrossRef]
Blume P, Wu S. Updating the diabetic foot treatment algorithm: recommendations on treatment using advanced medicine and therapies. Wounds. 2018;30(2):29–35.
Maier HM, Ilich JZ, Kim JS, Spicer MT. Nutrition supplementation for diabetic wound healing: a systematic review of current literature. Skinmed. 2013;11(4):217–24; quiz 224–5.
Arnold M, Barbul A. Nutrition and wound healing. Plast Reconstr Surg. 2006;117(7 Suppl):42S–58S. [CrossRef]
Chinese Diabetes Society, Society of Infectious Disease, Chinese Medical Association of Organization Repair and Regeneration Branch. [Chinese Guidelines for the Prevention and Treatment of Diabetic Foot (2019 edition)]. Chin J Diabetes. 2019;11:92–108. Chinese.
Shakil S, Khan AU. Infected foot ulcers in male and female diabetic patients: a clinico-bioinformative study. Ann Clin Microbiol Antimicrob. 2010;9:2. [CrossRef]
Yusof NM, Rahman JA, Zulkifly AH, Che-Ahmad A, Khalid KA, Sulong AF, et al. Predictors of major lower limb amputation among type II diabetic patients admitted for diabetic foot problems. Singapore Med J. 2015;56(11):626–31. [CrossRef]
Leung HB, Ho YC, Carnett J, Lam PK, Wong WC. Diabetic foot ulcers in the Hong Kong Chinese population: retrospective study. Hong Kong Med J. 2001;7(4):350–5.
Akinci B, Yener S, Yesil S, Yapar N, Kucukyavas Y, Bayraktar F. Acute phase reactants predict the risk of amputation in diabetic foot infection. J Am Podiatr Med Assoc. 2011;101(1):1–6. [CrossRef]
Xu S, Wang Y, Hu Z, Ma L, Zhang F, Liu P. Effects of neutrophil-tolymphocyte ratio, serum calcium, and serum albumin on prognosis in patients with diabetic foot. Int Wound J. 2023;20:1638–46.
Abstract
Keywords: Diabetic foot, infection, causative pathogens
Introduction
Diabetes mellitus is a major global health concern whose prevalence continues to increase steadily. One of its most serious complications is the development of foot ulcers, which represent a substantial cause of morbidity among affected individuals. Worldwide, a diabetes-related foot ulcer develops every 1–2 seconds, and a major amputation attributable to these wounds occurs approximately every 20 seconds (1). Among diabetes-related complications requiring hospitalization, diabetes-related foot infections remain the most common and continue to be the leading cause of lower-extremity amputation (2). Follow-up data from patients with diabetes-related foot infections indicate that, after 1 year, only 46% of ulcers have healed (with 10% of these subsequently recurring). In contrast, 15% of patients have died, and 17% have required lower-extremity amputation (3). These outcomes underscore that timely and appropriate infection management remains one of the most critical challenges in this patient population.
The spectrum of microorganisms responsible for diabetes-related foot infections can often be anticipated based on specific clinical factors. Superficial and mild infections are predominantly caused by Gram-positive bacteria, whereas advanced infections are more frequently associated with Gram-negative organisms; in cases accompanied by gangrene, anaerobic pathogens must also be considered (2,4). Particularly in advanced infections, Gram-positive, Gram-negative, and anaerobic organisms may coexist in a polymicrobial pattern (4). Moreover, interactions among these pathogens are clinically important, as they are associated with biofilm formation and the development of antimicrobial resistance (5).
In the absence of a life-threatening infection, the preferred approach is not to initiate empirical antibiotic therapy immediately, but rather to obtain appropriate tissue specimens and await microbiological results before selecting targeted antimicrobial treatment. Conversely, when a life-threatening infection is present, prompt empirical therapy should be initiated based on the most likely pathogens (6). When selecting empirical antibiotics, several factors must be carefully considered, including the availability of previous culture and susceptibility results from the same wound, the clinical severity of the infection, potential adverse effects of the selected agent, the need for dose adjustment according to renal and hepatic function, possible drug-drug interactions (particularly relevant given the high burden of comorbidities and concomitant medications in patients with diabetes), and overall treatment cost (7). In addition, knowledge of the regional distribution of causative pathogens, derived from prior studies, can substantially increase the likelihood of successful empirical therapy. For this reason, studies reporting the local microbiological profile of diabetes-related foot infections are of considerable importance, as they provide clinicians with essential data to guide treatment decisions.
The present study aimed to determine the distribution of causative pathogens among patients with diabetes-related foot infections treated as outpatients or inpatients at a secondary care hospital.
Materials and Methods
Study Design and Patient Selection
This retrospective study included patients who presented to the outpatient clinic or were hospitalized with a diagnosis of diabetes-related foot infection between May 1, 2025, and February 1, 2026.
Patients were eligible for inclusion if they met all of the following criteria:
- Age ≥ 18 years.
- Presentation to our hospital with a diagnosis of diabetes-related foot infection between May 1, 2025, and February 1, 2026.
- A diagnosis of infection was established according to the criteria defined by the International Working Group on the Diabetic Foot (IWGDF), including local signs of infection (swelling, erythema, increased local temperature, pain, purulent discharge) or systemic findings.
- Availability of tissue or aspiration samples obtained from the wound and sent to the microbiology laboratory for analysis.
- Availability of complete clinical and laboratory data in the electronic medical records.
Patients were excluded if they met any of the following criteria:
- Age < 18 years.
- Absence of tissue or aspiration sampling from the wound site.
- Incomplete or erroneous clinical or laboratory data.
- Presence of infections or foot lesions other than diabetes-related foot infections.
The study was approved by the Non-Interventional Clinical Research Ethics Committee of Aydın Adnan Menderes University Faculty of Medicine on March 26, 2026, with decision no. 2026/117.
Definition of Diabetes-related Foot Infection
The diagnosis of diabetes-related foot infection was established according to the criteria defined in the IWGDF guidelines (4). According to these criteria, infection was diagnosed in the presence of local signs of inflammation—such as swelling, erythema, increased local temperature, and pain—or systemic findings including fever, leukocytosis, and elevated C-reactive protein levels. The presence of purulent discharge from the wound and the clinician’s judgment that the lesion was infected were also considered diagnostic criteria.
Surgical Sampling Procedure
Under sterile conditions, any necrotic tissue present in the wound area was debrided using appropriate surgical techniques. Following adequate debridement, an adequate tissue specimen was obtained from the infected area and transported to the microbiology laboratory under sterile conditions for further analysis.
Microbiological Analyses
From the prepared fluid suspension of the specimen, 0.05 mL was inoculated onto 5% sheep blood agar and MacConkey agar plates using a sterile loop under aseptic conditions. The inoculated plates were incubated aerobically at 35°C and examined for microbial growth after 24 hours. If no growth was observed, the plates were re-incubated and reassessed at 48 hours post-inoculation.
Bacterial identification was performed using conventional biochemical methods. Upon detection of microbial growth, isolates were initially evaluated by Gram staining. Gram-negative organisms were identified based on standard biochemical characteristics, including glucose, sucrose, and lactose fermentation; citrate utilization; motility; urease and indole production; ornithine decarboxylase activity; and oxidase reaction. Gram-positive organisms were identified according to catalase activity, hemolytic patterns, coagulase production, susceptibility to optochin, bacitracin, and trimethoprim-sulfamethoxazole, as well as growth on bile esculin agar and in media containing 6.5% sodium chloride.
Antimicrobial susceptibility testing was performed and interpreted according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines. Identification of methicillin-resistant Staphylococcus aureus (MRSA) was performed using the cefoxitin disk diffusion method in accordance with EUCAST criteria. Each infection episode was analyzed as an independent event.
Results
A total of 197 patients were included in the study. Of these, 137 (69.5%) were male, and 60 (30.5%) were female. During the study period, 11 patients experienced a second infection episode. Overall, 208 wound specimens were obtained. No microbial growth was detected in 12 samples. Among the culture-positive specimens, 38 (18.3%) yielded two distinct infectious agents, indicating polymicrobial infection. In total, 196 culture-positive samples yielded 230 microbial isolates. Of these, 109 (47.4%) were Gram-positive organisms, and 119 (51.7%) were Gram-negative organisms (Table 1).
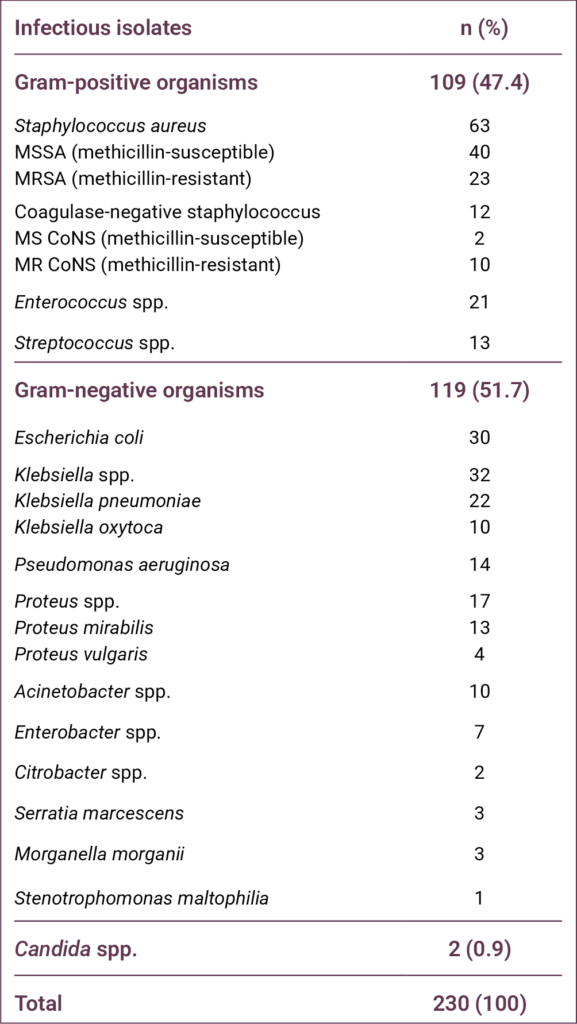
The most frequently isolated pathogen was S. aureus (n = 63, 27.4%), including 23 (10%) MRSA isolates. The second and third most common pathogens were Klebsiella spp. (n = 32, 13.9%) and Escherichia coli (n = 30, 13%), respectively.
Discussion
Studies conducted over the past several decades have demonstrated that the distribution of pathogens in patients with diabetes-related foot infections varies not only by region but also by country. When these studies are examined collectively, the world can be broadly categorized into two epidemiological regions. The first includes Europe and North America, where Gram-positive organisms predominate. The second comprises temperate regions encompassing Africa and Asia, where Gram-negative organisms are more prevalent, and the proportion of Pseudomonas aeruginosa is notably high (8). Studies conducted in Türkiye have generally indicated that the country aligns more closely with the second epidemiological pattern. For example, in a study covering a 15-year period, Gram-positive organisms accounted for 45.8% of isolates, whereas Gram-negative organisms accounted for 53.7% (9). In the same study, a statistically significant trend was observed over time, with Gram-positive pathogens increasing and Gram-negative pathogens decreasing. The distribution observed in our study was similar to these previously reported findings. Regarding specific pathogens, S. aureus, P. aeruginosa, and E. coli were consistently among the most frequently encountered organisms over the 15-year period, although their relative ranking varied by year (9). In a multicenter study by Acar et al. (10), which compared the pre–COVID-19 period with the pandemic period, a significant reduction in the number of specimens obtained for microbiological analysis during the pandemic was observed; however, no substantial change in pathogen distribution was identified. In that study, the most frequently isolated organisms were Pseudomonas spp. (16.4%) and S. aureus (15%) (10).
The findings of our study warrant particular discussion regarding P. aeruginosa. In the majority of studies conducted in Türkiye on diabetes-related foot infections, this pathogen has ranked either first or second among the most frequently isolated organisms (11–14). In contrast, in our study, P. aeruginosa ranked fifth. One important limitation of the existing literature in this field is that most studies have been conducted in tertiary-care hospitals, which may substantially influence pathogen distribution. Because our study was performed in a secondary-care state hospital, other Gram-negative organisms such as Klebsiella spp. (13.9%), E. coli (13%), and Proteus spp. (7.4%) may have become more prominent. Furthermore, Enterococcus spp. (9.1%), which has not been reported as a leading pathogen in several previous studies, was among the most frequently isolated organisms in our cohort.
Although an overall increase in Gram-positive pathogens has been observed in recent years in Türkiye, the proportion of S. aureus and, consequently, MRSA has reportedly declined. In a meta-analysis of studies conducted in Türkiye over the past two decades, the prevalence of S. aureus decreased from 29.4% to 18.1%, while the prevalence of MRSA declined from 12.5% to 5.5% (9). In that meta-analysis, the observed increase in Gram-positive organisms was primarily attributed to rising rates of Enterococcus spp. and Streptococcus spp. (9). In another recently published study presenting one-year data from five centers, the proportion of S. aureus was 14.6%, and the overall MRSA rate among all isolates was approximately 3% (15). In contrast to these reports, the proportion of S. aureus in our study was 27.4%, and the MRSA rate was 10%, both of which are considerably high. The elevated rates of S. aureus and MRSA observed in our cohort may indicate that pathogen distribution patterns in Türkiye are continuing to evolve. Nevertheless, our findings require confirmation through additional large-scale and multicenter studies.
Although relatively uncommon, fungal pathogens may also be implicated in diabetes-related foot infections, and pre-existing fungal infection of the foot or nails has been identified as a significant risk factor (16). In our study, Candida spp. was isolated from only two specimens, resulting in a very low prevalence.
The most important limitation of our study is the inability to evaluate anaerobic bacteria. Due to inadequate laboratory infrastructure, we were unable to assess the presence and distribution of anaerobic pathogens, which may represent a significant component of polymicrobial diabetes-related foot infections.
Conclusion
Our study revealed two key observations. First, the proportion of S. aureus and MRSA among patients presenting to our hospital with diabetes-related foot infections was relatively high. Second, although many studies conducted in Türkiye have reported a high prevalence of P. aeruginosa, this pathogen was not among the most frequently isolated organisms in our cohort. These results underscore the importance of local microbiological surveillance in guiding empirical antimicrobial therapy for diabetes-related foot infections. Further multicenter studies conducted in different regions are needed to confirm and expand upon these findings.
REFERENCES
Tentolouris N, Petrikkos G, Vallianou N, Zachos C, Daikos GL, Tsapogas P, et al. Prevalence of methicillin-resistant Staphylococcus aureus in infected and uninfected diabetic foot ulcers. Clin Microbiol Infect. 2006;12(2):186–9. [CrossRef]
Turhan V, Mutluoglu M, Acar A, Hatipoğlu M, Önem Y, Uzun G, et al. Increasing incidence of Gram-negative organisms in bacterial agents isolated from diabetic foot ulcers. J Infect Dev Ctries. 2013;7(10):707–12. [CrossRef]
Ndosi M, Wright-Hughes A, Brown S, Backhouse M, Lipsky BA, Bhogal M, et al. Prognosis of the infected diabetic foot ulcer: a 12-month prospective observational study. Diabet Med. 2018;35(1):78–88. [CrossRef]
Senneville E, Albalawi Z, van Asten SA, Abbas ZG, Allison G, Aragon-Sanchez J, et al. IWGDF/IDSA guidelines on the diagnosis and treatment of diabetes-related foot infections (IWGDF/IDSA 2023). Diabetes Metab Res Rev. 2024;40(3):e3687. [CrossRef]
Mitov I, Strateva T, Markova B. Prevalence of virulence genes among Bulgarian nosocomial and cystic fibrosis isolates of Pseudomonas aeruginosa. Braz J Microbiol. 2010;41(3):588–95. [CrossRef]
Ertugrul MB. [Medical therapy in diabetic foot infection]. TOTBID Derg. 2015;14(5):404–12. Turkish.
Ertuğrul B, Uçkay I, Schöni M, Peter-Riesch B, Lipsky BA. Management of diabetic foot infections in the light of recent literature and new international guidelines. Expert Rev Anti Infect Ther. 2020;18(4):293–305. [CrossRef]
Look DC, Stoll LL, Romig SA, Humlicek A, Britigan BE, Denning GM. Pyocyanin and its precursor phenazine-1-carboxylic acid increase IL-8 and intercellular adhesion molecule-1 expression in human airway epithelial cells by oxidant-dependent mechanisms. J Immunol. 2005;175(6):4017–23. [CrossRef]
Chantelau E, Kushner T, Spraul M. How effective is cushioned therapeutic footwear in protecting diabetic feet? A clinical study. Diabet Med. 1990;7(4):355–9. [CrossRef]
Acar A, Saltoğlu N, Tülek N, Turhan Ö, Serin EN, Yapar D, et al. Impact of the COVID-19 pandemic on diabetic foot patients: a shift in the infectious agent profile toward nonfermentative Gram-negative bacilli. J Am Podiatr Med Assoc. 2024;114(3):22–073. [CrossRef]
Ertugrul BM, Oncul O, Tulek N, Willke A, Sacar S, Tunccan OG, et al. A prospective, multi-center study: factors related to the management of diabetic foot infections. Eur J Clin Microbiol Infect Dis. 2012;31(9):2345–52. [CrossRef]
Ertugrul MB, Baktiroglu S, Salman S, Unal S, Aksoy M, Berberoglu K, et al. Pathogens isolated from deep soft tissue and bone in patients with diabetic foot infections. J Am Podiatr Med Assoc. 2008;98(4):290–5. [CrossRef]
Ertuğrul MB, Uyar-Güleç G, Baktıroğlu S, Çörekli E, Türe M. [The Distribution of Causative Microorganisms in Diabetic Foot Infection: Have There Been Any Alterations? ]. Klimik Derg. 2017;30(1):27–31. Turkish. [CrossRef]
Utlu Y, Başak O, Bozkurt-Kozan F, Ertuğrul MB. [Causative agents and factors associated with multidrug-resistant pathogens in diabetic foot infections]. Klimik Derg. 2019;32(1):84–9. Turkish. [CrossRef]
Gellatly SL, Hancock RE. Pseudomonas aeruginosa: new insights into pathogenesis and host defenses. Pathog Dis. 2013; 67(3):159–73. [CrossRef]
Bristow IR, Spruce MC. Fungal foot infection, cellulitis, and diabetes: a review. Diabet Med. 2009;26(5):548–51. [CrossRef]
Abstract
Keywords: Diabetic foot, quality of life, questionnaires, risk factors, foot ulcer, nursing care
Introduction
Diabetes mellitus (DM) is recognized as a major public health issue due to its rapidly increasing prevalence worldwide and the chronic complications it causes. Recent Global Burden of Disease analyses indicate that the prevalence of diabetes has increased substantially in recent decades and is projected to continue rising in the coming years (1). Data from the International Diabetes Federation (IDF) also highlight that diabetes imposes a significant clinical and economic burden on healthcare systems, in addition to its impact on individual health (2). Diabetic foot disease, one of the most serious complications of diabetes, is associated with increased morbidity, mortality, and healthcare costs. Among these complications, diabetic foot ulcers (DFUs) represent a major cause of prolonged hospitalization and permanent functional impairment. According to the current international guidelines, the management of such wounds requires a holistic approach that considers not only clinical healing but also the patient’s psychosocial well-being (3).
Diabetic foot ulcers are defined as chronic wounds that develop in individuals with diabetes, resulting from factors such as peripheral neuropathy and peripheral arterial disease. It is reported that approximately 19–34% of individuals with diabetes are at risk of developing DFUs during their lifetime. Current data indicate that DFUs affect millions of people worldwide (3). Diabetic foot disease is not merely a local wound problem but also carries serious systemic consequences. Indeed, five-year mortality rates among individuals with diabetic foot complications have been reported to be comparable to those observed in certain types of cancer (4). Furthermore, diabetic foot disease is one of the primary causes of non-traumatic lower-extremity amputations worldwide (2,5).
Diabetic foot ulcers are a significant problem not only in terms of clinical outcomes but also due to their negative impact on patients’ quality of life. Prolonged wound healing, pain, restricted mobility, recurrent infections, and repeated hospitalizations can significantly affect patients’ physical, psychological, and social well-being (6). Studies in the literature indicate that health-related quality of life (HRQoL) is markedly lower in individuals with DFUs (7–9). Furthermore, it has been reported that HRQoL may function not only as an outcome measure but also as a predictive factor of adverse clinical outcomes, including amputation and mortality (10).
Among the factors affecting quality of life in individuals with DFUs are numerous clinical and patient-related variables, such as ulcer severity, pain, infection, neuropathy, and metabolic control. In particular, loss of physical function and limitations in activities of daily living are major contributors to reduced quality of life (6,11). Therefore, patients with diabetic foot disease should be evaluated using a holistic approach that extends beyond wound management and incorporates quality-of-life assessment as an important clinical outcome.
There are limited studies examining the quality of life in patients with diabetic foot disease in Türkiye. Existing studies indicate that quality of life is low in patients with DFUs, particularly regarding physical functioning. A study conducted in Türkiye reported that patients with DFUs had significantly lower physical functioning scores compared with other individuals with diabetes, and that their overall quality-of-life levels were below societal norms (12). However, studies comprehensively examining the factors influencing quality of life in patients with diabetic foot disease remain limited.
Assessing quality of life in patients with diabetic foot disease is important not only for understanding patient well-being but also for predicting clinical outcomes and planning care pathways. Previous research has shown that poor quality of life may be associated with adverse outcomes, including amputation and mortality (10). Identifying the level of quality of life and its associated factors in patients with diabetic foot ulcers is important for developing patient-centered care strategies and improving clinical outcomes. Therefore, this study aimed to evaluate health-related quality of life (HRQoL) in patients with DFUs and to identify factors independently associated with HRQoL.
Materials and Methods
This multicenter, descriptive, cross-sectional study was conducted between August 2021 and August 2022 at the wound care clinic of a university hospital in the Southeastern Anatolia Region of Türkiye and the wound care unit of a private hospital in İstanbul.
The study population consisted of patients with DFUs who attended these wound care clinics during the specified period. A power analysis was performed to determine the sample size. Post-hoc power analysis was conducted for the final multiple linear regression model. Using the R² value of 0.158, the effect size (f²) was calculated as 0.188. Considering five independent variables, a significance level of α = 0.05, and the number of participants, the statistical power of the study was approximately 99%, indicating sufficient power to detect moderate effect sizes.
The inclusion criteria were age ≥18 years, a confirmed diagnosis of DFU, willingness to participate, and the cognitive capacity to provide informed consent. The exclusion criteria included a known diagnosis of psychotic disorder, schizophrenia, dementia, bipolar disorder, or intellectual disability; the presence of additional chronic conditions that could significantly affect quality of life and functional status; pregnancy; age <18 years; and refusal to participate. Written informed consent was obtained from all participants prior to data collection.
Data were collected by researchers through face-to-face interviews. Each interview lasted approximately 15–20 minutes and was completed in a single session.
The study was approved by the Clinical Non-Interventional Research Ethics Committee of SANKO University on July 7, 2021 with decision number 07/5.
Data Collection Tools
The Patient Information Form, developed by the researchers based on the literature, consisted of two sections. The first section included seven questions on sociodemographic characteristics, including gender, age, place of residence, educational status, marital status, employment status, and economic status (7,10).
The second section included 13 questions related to clinical and disease characteristics, such as type and duration of diabetes, duration of DFU treatment, history of previous DFUs, hemoglobin A1c level, presence of other chronic complications, Wagner classification stage, and presence of infection (7–10,13).
Ulcer severity was assessed using the Wagner Diabetic Foot Ulcer Classification, which categorizes ulcers from grade 0 to 5 based on ulcer depth, infection, and the presence of gangrene. Higher grades indicate greater ulcer depth and tissue damage (5).
Health-related quality of life was assessed using the Diabetic Foot Ulcer Scale–Short Form (DFS-SF), developed by Bann et al. (14). The Turkish validity and reliability study of the instrument was conducted by Kılıç et al. (15).
The DFS-SF consists of 29 items across six subscales: leisure time (L), physical health (PH), dependence/daily living (D/DL), negative emotions (NE), worry about feet/ulcers (WU/F), and discomfort regarding ulcer care.
It is a five-point Likert-type instrument ranging from “never” to “always.” Scores are transformed to a standardized 0–100 scale, with higher scores indicating better quality of life. No established cut-off value exists for the scale. In the Turkish validation study, the Cronbach’s alpha (α) coefficients for the subscales ranged from 0.93 to 0.97.
Statistical Analysis
Data were analyzed using SPSS Statistics version 22 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the data. The normality of continuous variables was assessed using skewness and kurtosis values, with values between ±1.5 considered acceptable for normal distribution. For comparisons between two groups, the independent samples t-test was used for normally distributed data, while the Mann-Whitney U test was applied for non-normally distributed variables. For comparisons involving more than two groups, one-way analysis of variance (ANOVA) or the Kruskal-Wallis test was used, depending on the distribution of the data. Post-hoc analyses were performed using the Tukey HSD test.
To identify factors associated with the total DFS-SF score, multivariate linear regression analysis was performed. Variables that were statistically significant in univariate analyses or considered clinically relevant were included in the initial model. A backward elimination procedure was used to remove nonsignificant variables and obtain the most parsimonious model.
Multicollinearity was assessed using the variance inflation factor (VIF) values. Model adequacy was evaluated using the coefficient of determination ( R² ) and the F test. A p-value of <0.05 was considered statistically significant.
Results
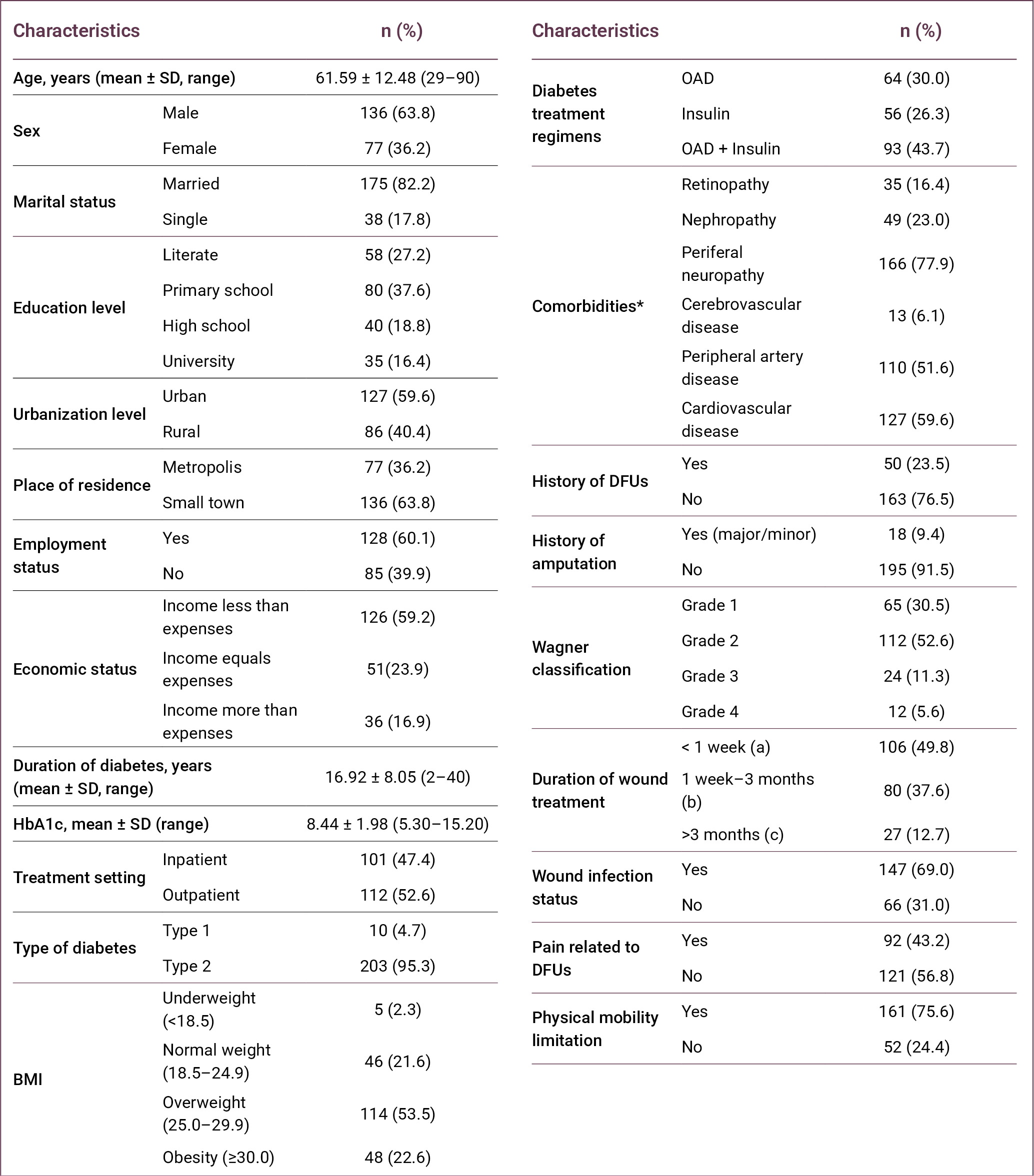
The mean age of the participants was 61.59 ± 12.48 years (range: 29–90), and 59.6% (n = 127) were younger than 65 years. Most participants were male (63.8%, n = 136) and married (82.2%, n = 175). The largest proportion of participants had a primary school education (37.6%; n = 80). In addition, 59.6% (n = 127) lived in urban areas, while 63.8% (n = 136) resided in small towns. More than half of the participants were employed (60.1%, n = 128), and 59.2% (n = 126) reported that their income was lower than their expenses (Table 1).
More than half of the participants received outpatient care (52.6%, n = 112), and the majority had type 2 diabetes (95.3%, n = 203). The mean duration of diabetes was 16.92 ± 8.05 years (range: 2–40). In terms of body mass index (BMI), 53.5% (n = 114) were classified as overweight. Regarding diabetes treatment, 43.7% (n = 93) were receiving a combination of oral antidiabetic drugs and insulin therapy.
Among comorbidities, peripheral neuropathy (77.9%; n = 166) and cardiovascular disease (59.6%; n = 127) were the most common. A history of diabetic foot ulcer was reported by 23.5% (n = 50) of participants, and 9.4% (n = 18) had a history of amputation. According to the Wagner classification, most participants were classified as grade 2 (52.6%; n = 112).
Regarding wound-related characteristics, 49.8% (n = 106) of the ulcers had been present for less than 1 week, and 69.0% (n = 147) were associated with infection. In addition, 43.2% (n = 92) of participants reported pain related to DFUs, and 75.6% (n = 161) had limitations in physical mobility.
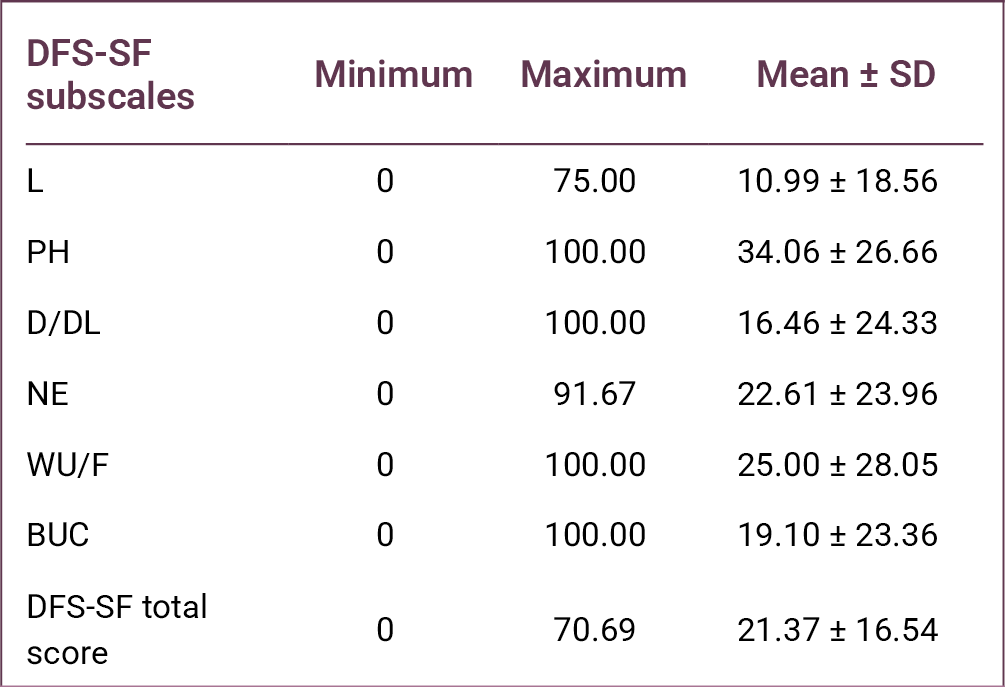
The mean DFS-SF total score was 21.37 ± 16.54, indicating substantially impaired HRQoL among patients with DFUs. Among the DFS-SF subscales, the highest mean score was observed in PH (34.06 ± 26.66), followed by WU/F (25.00 ± 28.05) and NE (22.61 ± 23.96). The lowest score was observed in the L subscale (10.99 ± 18.56) (Table 2).
When DFS-SF scores were analyzed according to sociodemographic characteristics, a statistically significant difference in total DFS-SF scores was found according to educational level (p = 0.036). Among the subscales, only the WU/F score differed significantly across educational groups (p = 0.015). Post-hoc Tukey analysis revealed that participants with primary school education had higher WU/F scores compared to literate individuals.
Significant differences were also observed according to place of residence, with differences detected in NE scores (p < 0.001) and DFS-SF total scores (p = 0.006). Similarly, urbanization level was associated with significant differences in NE, WU/F, and DFS-SF total scores (p = 0.018, p = 0.002, and p = 0.010, respectively).
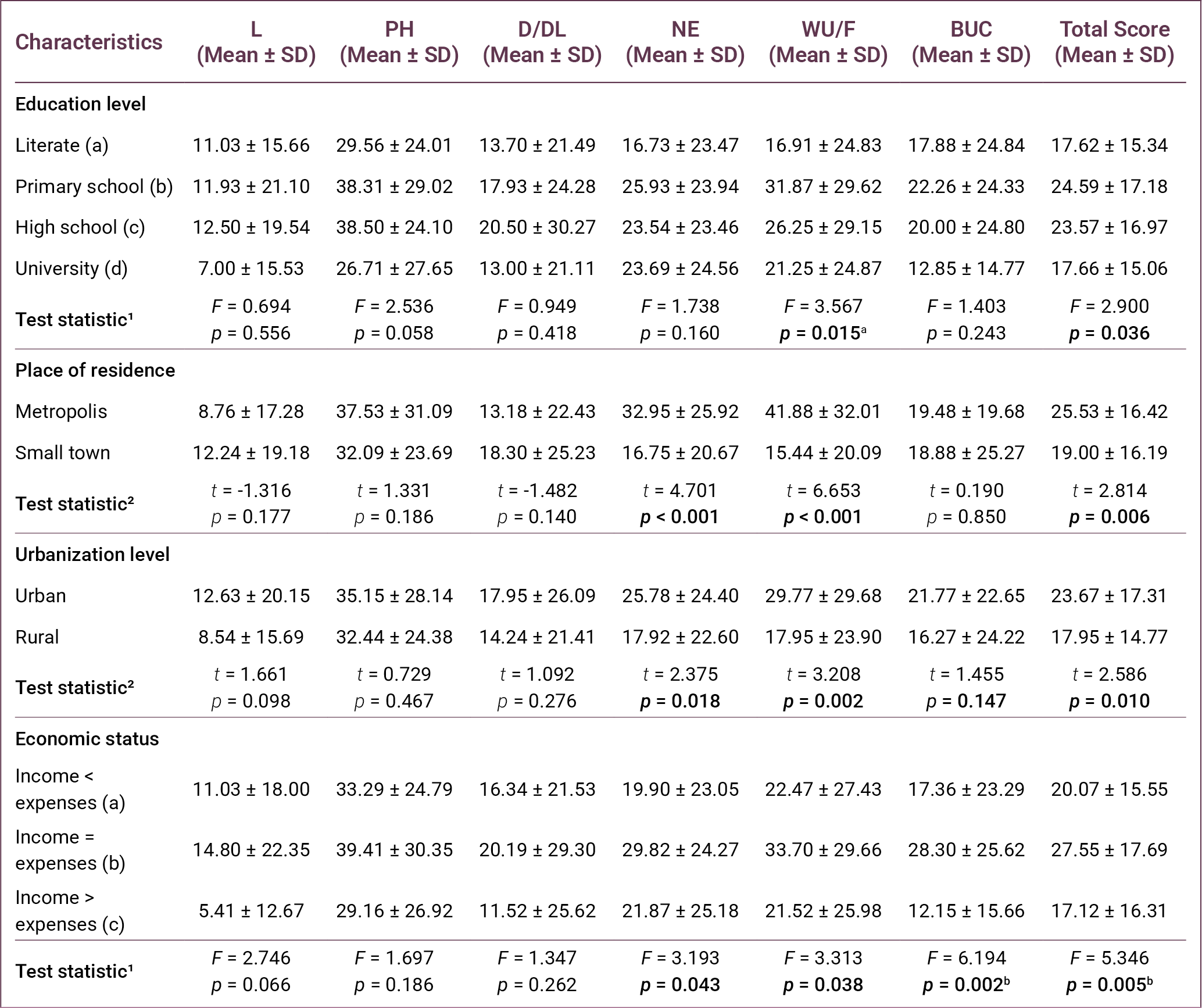
Regarding economic status, statistically significant differences were found in NE, WU/F, bothered by ulcer care (BUC), and total DFS-SF scores (p = 0.043, p = 0.038, p = 0.002, and p = 0.005, respectively). Post-hoc analysis demonstrated that participants whose income equaled their expenses had higher WU/F and BUC scores compared with those whose income exceeded their expenses. Additionally, participants whose income equaled their expenses had higher total DFS-SF scores than those whose income was lower than their expenses (Table 3).
As presented in Table 4, comparisons based on treatment setting showed significant differences in L, NE, WU/F, and BUC scores (p = 0.001, p = 0.004, p < 0.001, and p = 0.042, respectively). Patients without nephropathy demonstrated significantly higher scores in PH, NE, WU/F, and total DFS-SF scores (p = 0.033, p = 0.023, p < 0.001, and p = 0.002, respectively).
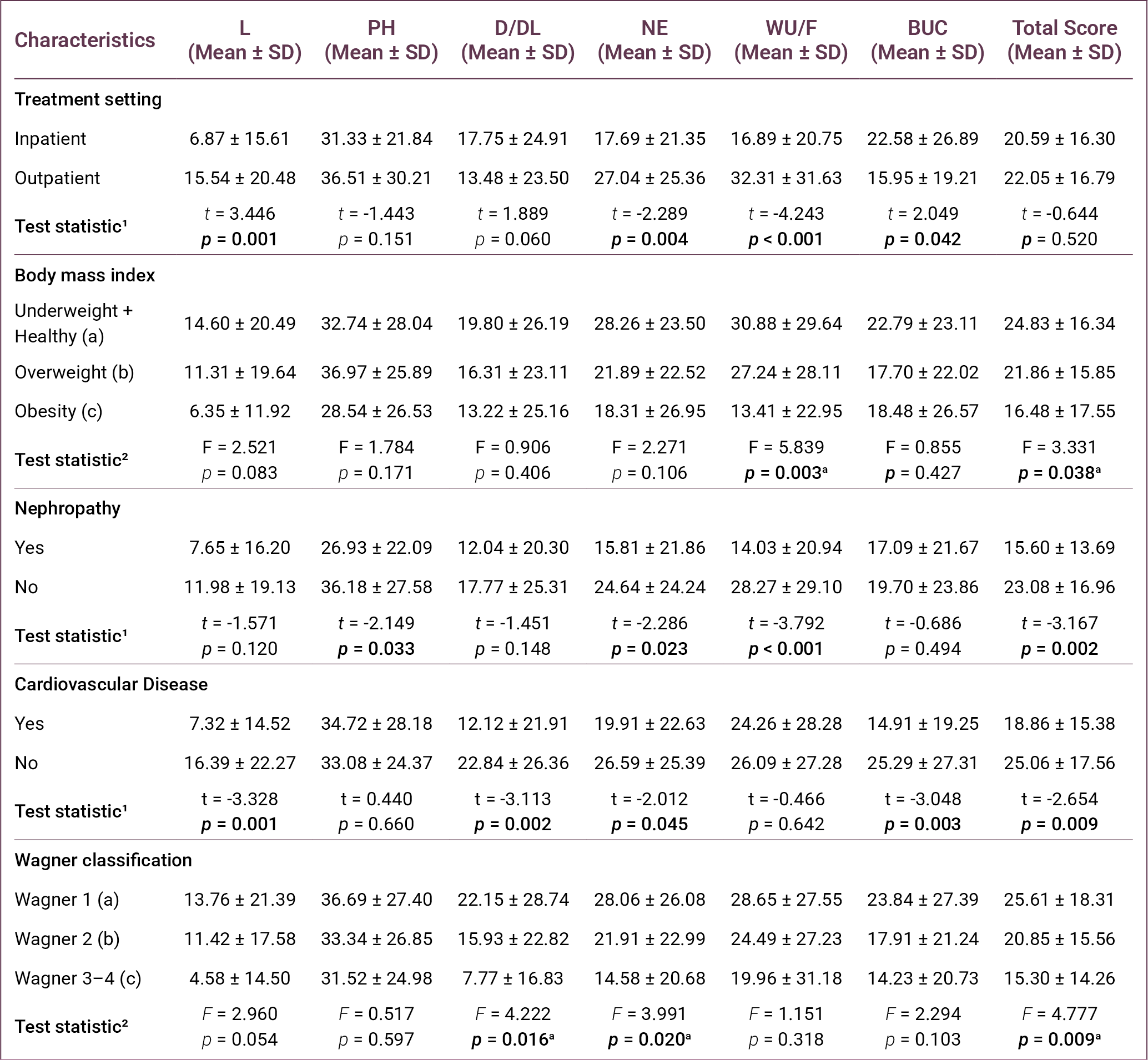
With respect to cardiovascular disease, significant differences were observed in L, D/DL, NE, BUC, and DFS-SF total scores (p = 0.001, p = 0.002, p = 0.045, p = 0.003, and p = 0.009, respectively).
According to the Wagner classification, statistically significant differences were found in D/DL, NE, and total DFS-SF scores (p = 0.016, p = 0.020, and p = 0.009, respectively). Post-hoc Tukey analysis indicated that patients in Wagner stage 1 ulcers had higher scores compared to those with stages 2 and 3–4.
As presented in Table 5, comparisons according to ulcer- and symptom-related characteristics showed statistically significant differences in WU/F and BUC scores according to a history of DFUs (p = 0.002 and p = 0.011, respectively).
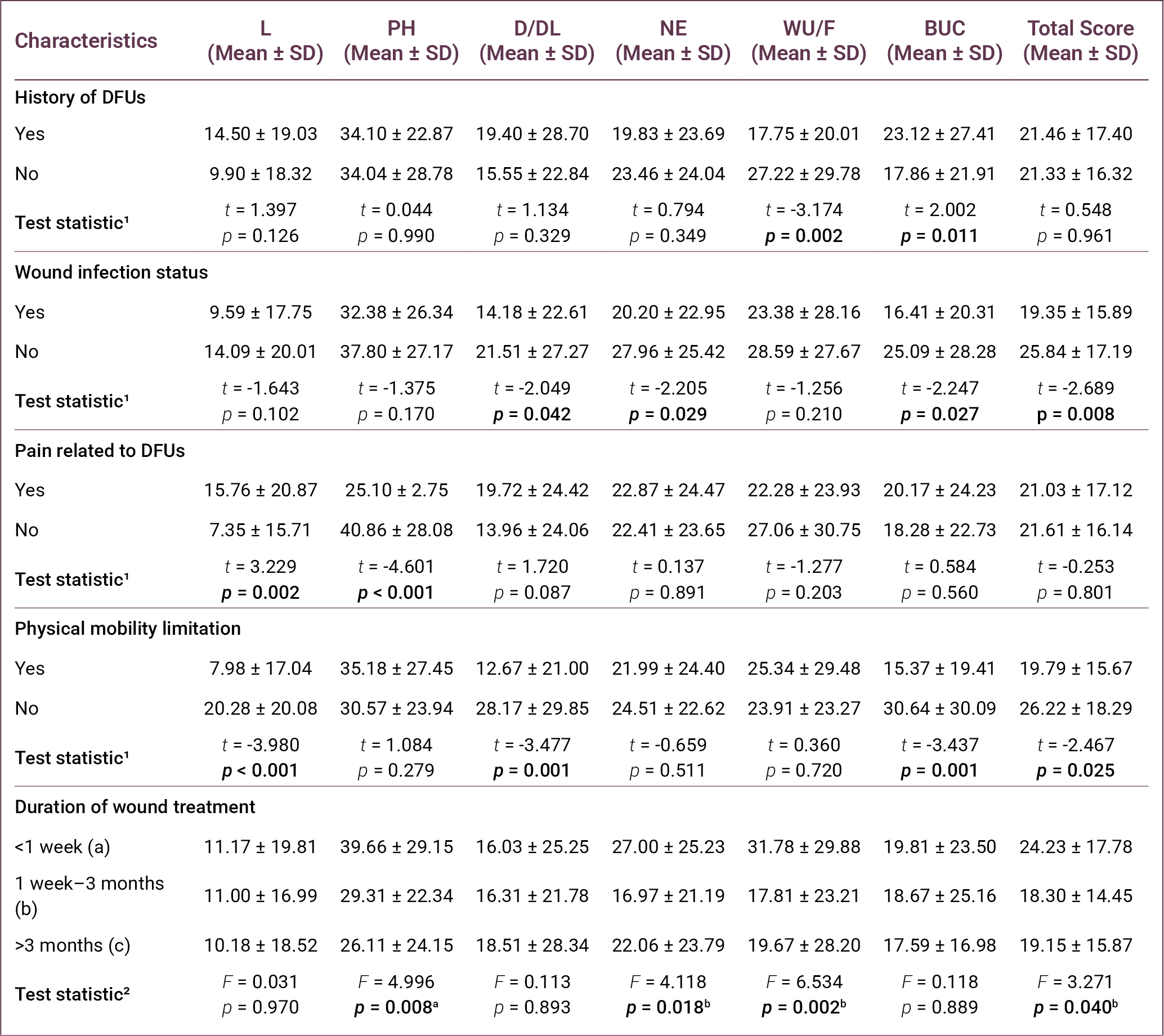
Significant differences were also observed in D/DL, NE, BUC, and total DFS-SF scores according to the presence of wound infection (p = 0.042, p = 0.029, p = 0.027, and p = 0.008, respectively).
In terms of pain related to DFUs, significant differences were found in L and PH scores (p = 0.002 and p < 0.001, respectively). Similarly, physical mobility limitation was associated with significant differences in L, D/DL, BUC, and total DFS-SF scores (p < 0.001, p = 0.001, p = 0.001, and p = 0.025, respectively).
Regarding duration of wound treatment, statistically significant differences were found in PH, NE, WU/F, and DFS-SF total scores ( p = 0.008, p = 0.018, p = 0.002, and p = 0.040, respectively). Post-hoc analysis indicated that participants with wound durations of less than 1 week had higher scores than those with longer wound durations.
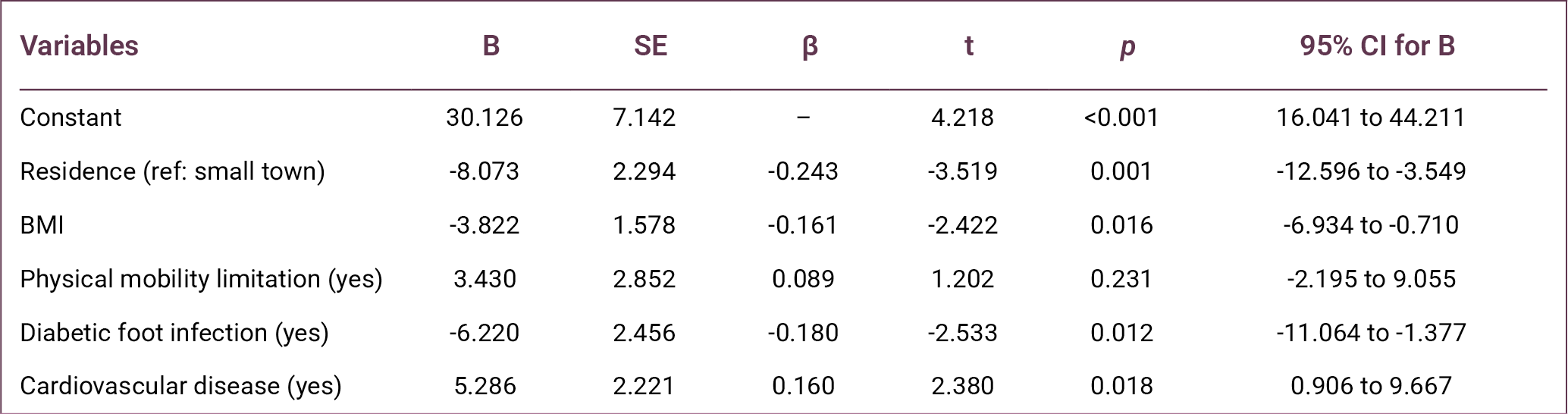
Finally, multivariate linear regression analysis was performed to identify independent factors associated with the DFS-SF total score. The regression model was statistically significant (F = 7.390, p < 0.001) and explained 15.8% of the variance in the DFS-SF total score (R² = 0.158).
The analysis revealed that place of residence (β = -0.243, p = 0.001), BMI (β=-0.161, p = 0.016), presence of diabetic foot infection (β=-0.180, p = 0.012), and presence of cardiovascular disease (β = 0.160, p = 0.018) were independent factors associated with the DFS-SF total score (Table 6).
Discussion
This study demonstrated that HRQoL is markedly impaired in individuals with DFUs, indicating that DFUs represent not only a clinical condition but also a multidimensional burden affecting physical, functional, and psychosocial domains. The low DFS-SF scores observed across all subscales, particularly in L and D/DL, highlight the substantial restrictions imposed by the disease on patients’ everyday functioning.
A prospective cohort study conducted in Singapore reported that HRQoL was low at baseline in patients with DFUs, with an EuroQol 5-Dimension (EQ-5D) utility value of 0.736 (9). Similarly, the Eurodiale study demonstrated that quality of life in patients presenting with DFUs was significantly affected, particularly in the areas of mobility and pain/discomfort (10). In a study conducted by Lima Neto et al. (16) in Brazil, scores on most subscales of the SF-36 quality of life questionnaire were reported to be low in individuals with DFUs, with the “physical role limitations” domain being the most affected. Likewise, Sekhar et al. (11) showed that both physical and mental quality-of-life scores were significantly lower in patients with DFUs compared with individuals without diabetic foot. Furthermore, a meta-analysis involving adults with DFUs reported markedly lower quality of life, particularly in the domains of physical functioning, physical role, general health, and vitality (7). Together, these findings consistently demonstrate that DFUs negatively affect quality of life across multiple dimensions.
In the present study, the relatively low quality-of-life scores may be explained by the clinical characteristics of the study population. A considerable proportion of participants experienced mobility limitation (75.6%), wound infection (69.0%), and DFU-related pain (43.2%), all of which are known to negatively affect physical functioning and daily activities. Additionally, the relatively high mean age of the participants (61.59 ± 12.48), with approximately 40% aged ≥65 years, may have contributed to the lower HRQoL observed. Advanced age is often associated with increased comorbidity burden, reduced physical capacity, and delayed wound healing, which may lead to a greater impact on quality of life in patients with DFU (8,17).
Consistent with previous studies, ulcer severity emerged as a key determinant of HRQoL in this study. The progressive decline in quality-of-life scores with increasing Wagner stage suggests that disease progression is closely linked to worsening functional status and symptom burden. Advanced-stage ulcers are typically associated with higher infection risk, prolonged treatment duration, and increased likelihood of hospitalization or amputation, all of which may impair patients’ physical and psychological well-being.
Similar findings have been reported in previous research. Alrub et al. (18) demonstrated that patients with lower Wagner stages reported significantly higher quality-of-life scores. Likewise, Kudlová and Kočvarová (8) reported that ulcer depth and clinical severity are associated with quality of life in individuals with DFUs. A systematic review examining the impact of diabetic foot complications also concluded that advanced-stage ulcers cause more pronounced deterioration in quality of life (19). Furthermore, a meta-analysis of DFU studies reported that larger wounds were associated with a significant decline in quality of life (7). These findings support the notion that ulcer severity is one of the key clinical indicators determining quality of life in patients with DFUs.
Mobility limitation was another critical factor associated with poorer HRQoL. A large proportion of participants experienced restricted physical movement, suggesting that loss of independence is a central component of the disease burden in DFUs. Reduced mobility may limit participation in daily and social activities, thereby negatively affecting both physical and emotional aspects of quality of life. Previous research also highlights the importance of mobility in determining HRQoL. The Eurodiale study reported that inability to walk or dependence on others for daily activities was associated with a marked decline in quality of life across many domains (10). Similarly, studies have shown that mobility limitations negatively affect physical functioning and activities of daily living in patients with diabetic foot problems (16,20,21). These findings highlight the importance of incorporating rehabilitation strategies and mobility-preserving interventions into DFU management.
This study also highlights the role of clinical complications, particularly infection and comorbid conditions. Diabetic foot infection was identified as an independent predictor of lower HRQoL, likely reflecting its association with pain, inflammation, and treatment complexity. Similarly, the presence of cardiovascular disease was associated with reduced quality of life, possibly due to decreased physical capacity and increased overall disease burden.
Multivariate regression analysis identified place of residence, BMI, diabetic foot infection, and cardiovascular disease as independent predictors of quality of life. In particular, place of residence was found to be one of the strongest predictors (β = -0.243, p = 0.001). This finding indicates that HRQoL in patients with diabetic foot disease is influenced not only by clinical factors but also by socioeconomic and environmental conditions, such as access to healthcare services, availability of social support, and healthcare infrastructure (21).
Individuals living in large cities had lower quality-of-life scores in this study. This finding may reflect differences in living conditions, the burden of disease, social support networks, and access to healthcare services in large cities. However, this finding needs to be clarified by further studies. Furthermore, lower educational and economic status were associated with poorer quality of life, which may be explained by differences in health literacy, self-care behaviors, and access to healthcare resources (13).
Body mass index was also negatively associated with HRQoL (β = -0.161, p = 0.016). Higher BMI may worsen outcomes in patients with DFUs through mechanisms such as reduced mobility, increased plantar pressure, delayed wound healing, and difficulties in implementing effective off-loading strategies (7). Consequently, obesity may exacerbate both ulcer formation and the wound-healing process while simultaneously limiting physical functioning and independence. These findings underscore the importance of integrating weight management strategies into comprehensive DFU care.
Diabetic foot infection was also identified as an independent determinant of HRQoL (β = -0.180, p = 0.012). Infection may negatively affect patients’ physical and psychosocial well-being through pain, inflammation, prolonged treatment duration, and increased need for hospitalization (22). Similarly, the decisive role of infection on quality of life is also emphasized in the literature (10,23). Consequently, early diagnosis and effective management of infection are essential not only for clinical recovery but also for preserving patients’ quality of life.
The presence of cardiovascular disease was identified as an independent determinant of quality of life. Cardiovascular diseases can negatively affect quality of life in patients with diabetic foot through mechanisms such as peripheral circulatory disorders, reduced physical capacity and functional limitations (14,23). The fact that cardiovascular diseases reduce physical capacity and lead to functional limitations may contribute to a decline in quality of life in patients with diabetic foot. Furthermore, the identification of the presence of cardiovascular disease as one of the independent determinants of quality of life in the regression analysis in this study supports the importance of this relationship.
Although the regression model explained a modest proportion of variance in HRQoL, this finding suggests that additional psychological, behavioral, and healthcare-related factors may also contribute to patient outcomes. Nevertheless, the predictors identified in this study provide clinically relevant targets for intervention.
Overall, these findings indicate that improving HRQoL in patients with DFUs requires a comprehensive and multidisciplinary approach. Beyond wound care, effective management should include infection control, management of comorbidities, mobility support, and attention to socioenvironmental determinants of health. Such integrated care strategies may enhance both clinical outcomes and patient-reported quality of life.
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between variables. Second, the sample was recruited from two healthcare centers, which may limit the generalizability of the findings. Third, quality of life was assessed using self-reported measures, which may introduce response bias. In addition, the cross-sectional design did not allow evaluation of longitudinal changes in HRQoL over time. Despite these limitations, the inclusion of participants from two different clinical centers enhances the clinical relevance of the findings. Future multicenter and longitudinal studies are needed to better understand the determinants of HRQoL in patients with DFUs.
In conclusion, this study demonstrates that HRQoL is generally impaired among individuals with DFUs and is influenced by both clinical and sociodemographic factors. Ulcer severity, diabetic foot infection, mobility limitations, BMI, and comorbid cardiovascular disease were associated with poorer HRQoL, while place of residence emerged as an important socioenvironmental determinant. Our findings highlight the multidimensional burden of DFUs and emphasize the need for early identification and management of modifiable risk factors. Further longitudinal research is needed to better understand the long-term impact of these interventions on quality of life.
REFERENCES
GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–34. Erratum in: Lancet. 2023;402(10408):1132. Erratum in: Lancet. 2025;405(10474):202. [CrossRef]
International Diabetes Federation. IDF annual report 2024 [Internet]. Brussels: International Diabetes Federation; 2024. [cited March 24, 2026]. Available from: https://idf.org
Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA. 2023;330(1):62–75. [CrossRef]
Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. [CrossRef]
Schaper NC, van Netten JJ, Apelqvist J, Bus SA, Fitridge R, Game F, et al; IWGDF Editorial Board. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3657. [CrossRef]
Navarro-Flores E, Cauli O. Quality of life in ındividuals with diabetic foot syndrome. Endocr Metab Immune Disord Drug Targets. 2020;20(9):1365–72. [CrossRef]
Khunkaew S, Fernandez R, Sim J. Health-related quality of life among adults living with diabetic foot ulcers: a meta-analysis. Qual Life Res. 2019;28(6):1413–27. [CrossRef]
Kudlová P, Kočvarová I. Quality of life in patients with diabetic foot ulcers. Cent Eur J Nurs Midw. 2020;11(1):34–42. [CrossRef]
Lam BJW, Lee PYF, Liew H, et al. Health-related quality of life of patients with diabetic foot ulcers in Singapore: A cross-sectional and longitudinal analysis. Proc Singap Healthc. 2025;34. [CrossRef]
Siersma V, Thorsen H, Holstein PE, Kars M, Apelqvist J, Jude EB, et al. Health-related quality of life predicts major amputation and death, but not healing, in people with diabetes presenting with foot ulcers: the Eurodiale study. Diabetes Care. 2014;37(3):694–700. [CrossRef]
Sekhar MS, Thomas RR, Unnikrishnan MK, Vijayanarayana K, Rodrigues GS. Impact of diabetic foot ulcer on health-related quality of life: A cross-sectional study. Semin Vasc Surg. 2015;28(3-4):165–71. [CrossRef]
Kuman Tunçel Ö, Mert M, Erdem HA, Öztürk AM, Vahabi A, Şanlıdağ G, et al. [The quality of life in the patients with diabetic foot ulcers]. FLORA. 2021;26(2):295–302. Turkish. [CrossRef]
Kolarić V, Svirčević V, Bijuk R, Zupančič V. Chronic complications of diabetes and quality of life. Acta Clin Croat. 2022;61(3):520–7. [CrossRef]
Bann CM, Fehnel SE, Gagnon DD. Development and validation of the Diabetic Foot Ulcer Scale-short form (DFS-SF). Pharmacoeconomics. 2003;21(17):1277–90. [CrossRef]
Kiliç M, Karadağ A, Koçakgöl N. The validity and reliability of the Diabetic Foot Scale-Short Form (DFS-SF) in the Turkish population: a methodological study. Turk J Med Sci. 2023;53(5):1438–47. [CrossRef]
Lima Neto PM, Lima PHS, Santos FDRP, Jesus LMS, Lima RJCP, Santos LH. Quality of life of people with diabetic foot. Rev Rene. 2016;17(2):191–7. [CrossRef]
Nemcová J, Hlinková E, Farský I, Žiaková K, Jarošová D, Zeleníková R, et al. Quality of life in patients with diabetic foot ulcer in Visegrad countries. J Clin Nurs. 2017;26(9-10):1245–56. [CrossRef]
Alrub AA, Hyassat D, Khader YS, Bani-Mustafa R, Younes N, Ajlouni K. Factors associated with health-related quality of life among Jordanian patients with diabetic foot ulcer. J Diabetes Res. 2019;2019:4706720. [CrossRef]
Eroğlu N. [Diabetic foot problems in diabetic patients effect on quality of life: systematic review]. J Nurs Sci. 2018;1(2):19–22. Turkish.
Sothornwit J, Srisawasdi G, Suwannakin A, Sriwijitkamol A. Decreased health-related quality of life in patients with diabetic foot problems. Diabetes Metab Syndr Obes. 2018;11:35–43. [CrossRef]
Stasini FB, Margari N, Fasoi G, Kelesi M, Dafogianni C. Quality of life among patients with diabetic foot ulcer. Int J Caring Sci. 2020;13(2):1073–80.
Raspovic KM, Wukich DK. Self-reported quality of life and diabetic foot infections. J Foot Ankle Surg. 2014;53(6):716–9. [CrossRef]
Oe M, Saad SS, Jais S, Sugama J. Impact of foot ulcer-related factors on quality of life in patients with diabetes: Prospective observational study. Int Wound J. 2024;21(5):e14895. [CrossRef]