
Abstract
Keywords: Diabetic foot, quality of life, questionnaires, risk factors, foot ulcer, nursing care
Introduction
Diabetes mellitus (DM) is recognized as a major public health issue due to its rapidly increasing prevalence worldwide and the chronic complications it causes. Recent Global Burden of Disease analyses indicate that the prevalence of diabetes has increased substantially in recent decades and is projected to continue rising in the coming years (1). Data from the International Diabetes Federation (IDF) also highlight that diabetes imposes a significant clinical and economic burden on healthcare systems, in addition to its impact on individual health (2). Diabetic foot disease, one of the most serious complications of diabetes, is associated with increased morbidity, mortality, and healthcare costs. Among these complications, diabetic foot ulcers (DFUs) represent a major cause of prolonged hospitalization and permanent functional impairment. According to the current international guidelines, the management of such wounds requires a holistic approach that considers not only clinical healing but also the patient’s psychosocial well-being (3).
Diabetic foot ulcers are defined as chronic wounds that develop in individuals with diabetes, resulting from factors such as peripheral neuropathy and peripheral arterial disease. It is reported that approximately 19–34% of individuals with diabetes are at risk of developing DFUs during their lifetime. Current data indicate that DFUs affect millions of people worldwide (3). Diabetic foot disease is not merely a local wound problem but also carries serious systemic consequences. Indeed, five-year mortality rates among individuals with diabetic foot complications have been reported to be comparable to those observed in certain types of cancer (4). Furthermore, diabetic foot disease is one of the primary causes of non-traumatic lower-extremity amputations worldwide (2,5).
Diabetic foot ulcers are a significant problem not only in terms of clinical outcomes but also due to their negative impact on patients’ quality of life. Prolonged wound healing, pain, restricted mobility, recurrent infections, and repeated hospitalizations can significantly affect patients’ physical, psychological, and social well-being (6). Studies in the literature indicate that health-related quality of life (HRQoL) is markedly lower in individuals with DFUs (7–9). Furthermore, it has been reported that HRQoL may function not only as an outcome measure but also as a predictive factor of adverse clinical outcomes, including amputation and mortality (10).
Among the factors affecting quality of life in individuals with DFUs are numerous clinical and patient-related variables, such as ulcer severity, pain, infection, neuropathy, and metabolic control. In particular, loss of physical function and limitations in activities of daily living are major contributors to reduced quality of life (6,11). Therefore, patients with diabetic foot disease should be evaluated using a holistic approach that extends beyond wound management and incorporates quality-of-life assessment as an important clinical outcome.
There are limited studies examining the quality of life in patients with diabetic foot disease in Türkiye. Existing studies indicate that quality of life is low in patients with DFUs, particularly regarding physical functioning. A study conducted in Türkiye reported that patients with DFUs had significantly lower physical functioning scores compared with other individuals with diabetes, and that their overall quality-of-life levels were below societal norms (12). However, studies comprehensively examining the factors influencing quality of life in patients with diabetic foot disease remain limited.
Assessing quality of life in patients with diabetic foot disease is important not only for understanding patient well-being but also for predicting clinical outcomes and planning care pathways. Previous research has shown that poor quality of life may be associated with adverse outcomes, including amputation and mortality (10). Identifying the level of quality of life and its associated factors in patients with diabetic foot ulcers is important for developing patient-centered care strategies and improving clinical outcomes. Therefore, this study aimed to evaluate health-related quality of life (HRQoL) in patients with DFUs and to identify factors independently associated with HRQoL.
Materials and Methods
This multicenter, descriptive, cross-sectional study was conducted between August 2021 and August 2022 at the wound care clinic of a university hospital in the Southeastern Anatolia Region of Türkiye and the wound care unit of a private hospital in İstanbul.
The study population consisted of patients with DFUs who attended these wound care clinics during the specified period. A power analysis was performed to determine the sample size. Post-hoc power analysis was conducted for the final multiple linear regression model. Using the R² value of 0.158, the effect size (f²) was calculated as 0.188. Considering five independent variables, a significance level of α = 0.05, and the number of participants, the statistical power of the study was approximately 99%, indicating sufficient power to detect moderate effect sizes.
The inclusion criteria were age ≥18 years, a confirmed diagnosis of DFU, willingness to participate, and the cognitive capacity to provide informed consent. The exclusion criteria included a known diagnosis of psychotic disorder, schizophrenia, dementia, bipolar disorder, or intellectual disability; the presence of additional chronic conditions that could significantly affect quality of life and functional status; pregnancy; age <18 years; and refusal to participate. Written informed consent was obtained from all participants prior to data collection.
Data were collected by researchers through face-to-face interviews. Each interview lasted approximately 15–20 minutes and was completed in a single session.
The study was approved by the Clinical Non-Interventional Research Ethics Committee of SANKO University on July 7, 2021 with decision number 07/5.
Data Collection Tools
The Patient Information Form, developed by the researchers based on the literature, consisted of two sections. The first section included seven questions on sociodemographic characteristics, including gender, age, place of residence, educational status, marital status, employment status, and economic status (7,10).
The second section included 13 questions related to clinical and disease characteristics, such as type and duration of diabetes, duration of DFU treatment, history of previous DFUs, hemoglobin A1c level, presence of other chronic complications, Wagner classification stage, and presence of infection (7–10,13).
Ulcer severity was assessed using the Wagner Diabetic Foot Ulcer Classification, which categorizes ulcers from grade 0 to 5 based on ulcer depth, infection, and the presence of gangrene. Higher grades indicate greater ulcer depth and tissue damage (5).
Health-related quality of life was assessed using the Diabetic Foot Ulcer Scale–Short Form (DFS-SF), developed by Bann et al. (14). The Turkish validity and reliability study of the instrument was conducted by Kılıç et al. (15).
The DFS-SF consists of 29 items across six subscales: leisure time (L), physical health (PH), dependence/daily living (D/DL), negative emotions (NE), worry about feet/ulcers (WU/F), and discomfort regarding ulcer care.
It is a five-point Likert-type instrument ranging from “never” to “always.” Scores are transformed to a standardized 0–100 scale, with higher scores indicating better quality of life. No established cut-off value exists for the scale. In the Turkish validation study, the Cronbach’s alpha (α) coefficients for the subscales ranged from 0.93 to 0.97.
Statistical Analysis
Data were analyzed using SPSS Statistics version 22 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize the data. The normality of continuous variables was assessed using skewness and kurtosis values, with values between ±1.5 considered acceptable for normal distribution. For comparisons between two groups, the independent samples t-test was used for normally distributed data, while the Mann-Whitney U test was applied for non-normally distributed variables. For comparisons involving more than two groups, one-way analysis of variance (ANOVA) or the Kruskal-Wallis test was used, depending on the distribution of the data. Post-hoc analyses were performed using the Tukey HSD test.
To identify factors associated with the total DFS-SF score, multivariate linear regression analysis was performed. Variables that were statistically significant in univariate analyses or considered clinically relevant were included in the initial model. A backward elimination procedure was used to remove nonsignificant variables and obtain the most parsimonious model.
Multicollinearity was assessed using the variance inflation factor (VIF) values. Model adequacy was evaluated using the coefficient of determination ( R² ) and the F test. A p-value of <0.05 was considered statistically significant.
Results
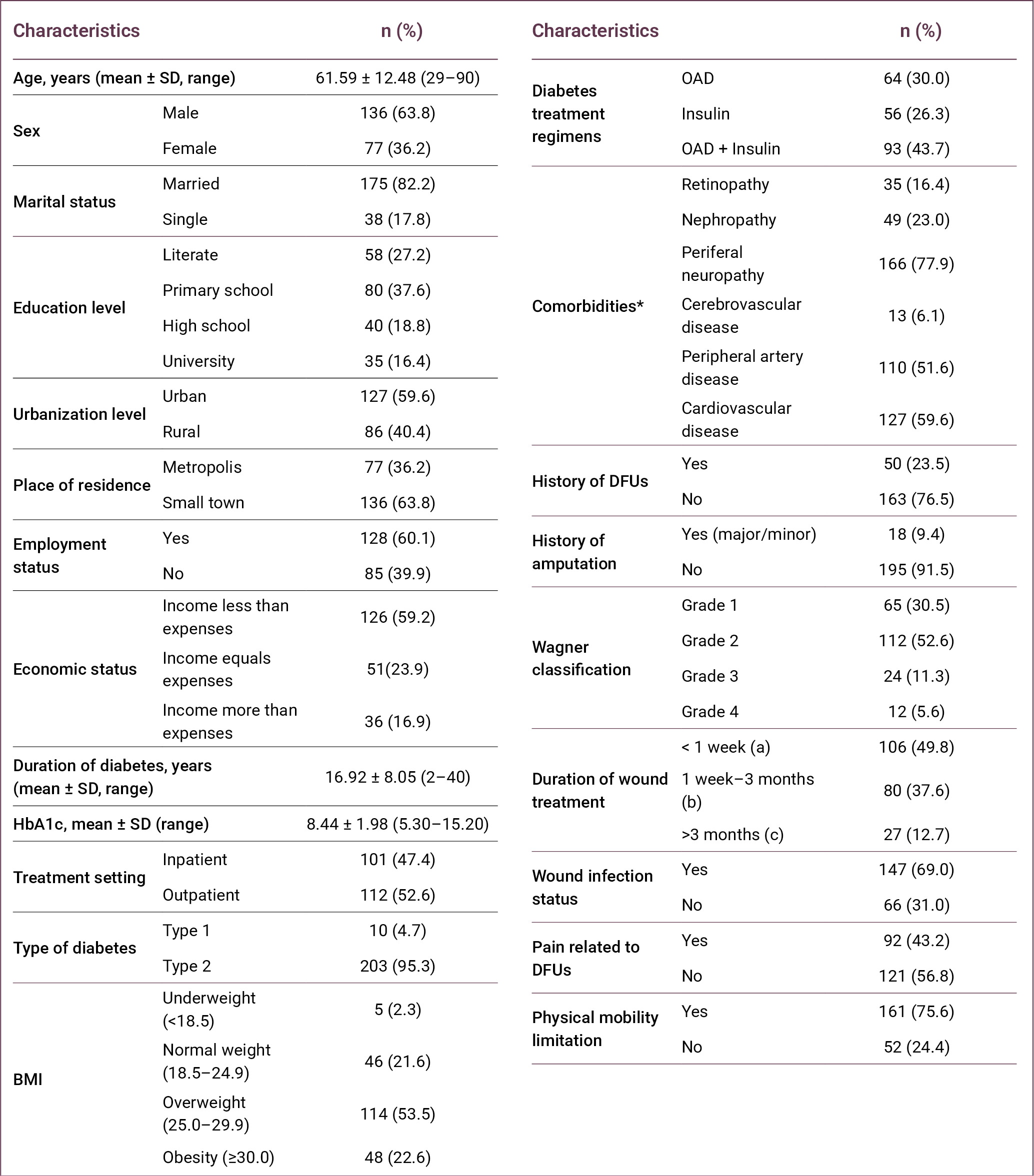
The mean age of the participants was 61.59 ± 12.48 years (range: 29–90), and 59.6% (n = 127) were younger than 65 years. Most participants were male (63.8%, n = 136) and married (82.2%, n = 175). The largest proportion of participants had a primary school education (37.6%; n = 80). In addition, 59.6% (n = 127) lived in urban areas, while 63.8% (n = 136) resided in small towns. More than half of the participants were employed (60.1%, n = 128), and 59.2% (n = 126) reported that their income was lower than their expenses (Table 1).
More than half of the participants received outpatient care (52.6%, n = 112), and the majority had type 2 diabetes (95.3%, n = 203). The mean duration of diabetes was 16.92 ± 8.05 years (range: 2–40). In terms of body mass index (BMI), 53.5% (n = 114) were classified as overweight. Regarding diabetes treatment, 43.7% (n = 93) were receiving a combination of oral antidiabetic drugs and insulin therapy.
Among comorbidities, peripheral neuropathy (77.9%; n = 166) and cardiovascular disease (59.6%; n = 127) were the most common. A history of diabetic foot ulcer was reported by 23.5% (n = 50) of participants, and 9.4% (n = 18) had a history of amputation. According to the Wagner classification, most participants were classified as grade 2 (52.6%; n = 112).
Regarding wound-related characteristics, 49.8% (n = 106) of the ulcers had been present for less than 1 week, and 69.0% (n = 147) were associated with infection. In addition, 43.2% (n = 92) of participants reported pain related to DFUs, and 75.6% (n = 161) had limitations in physical mobility.
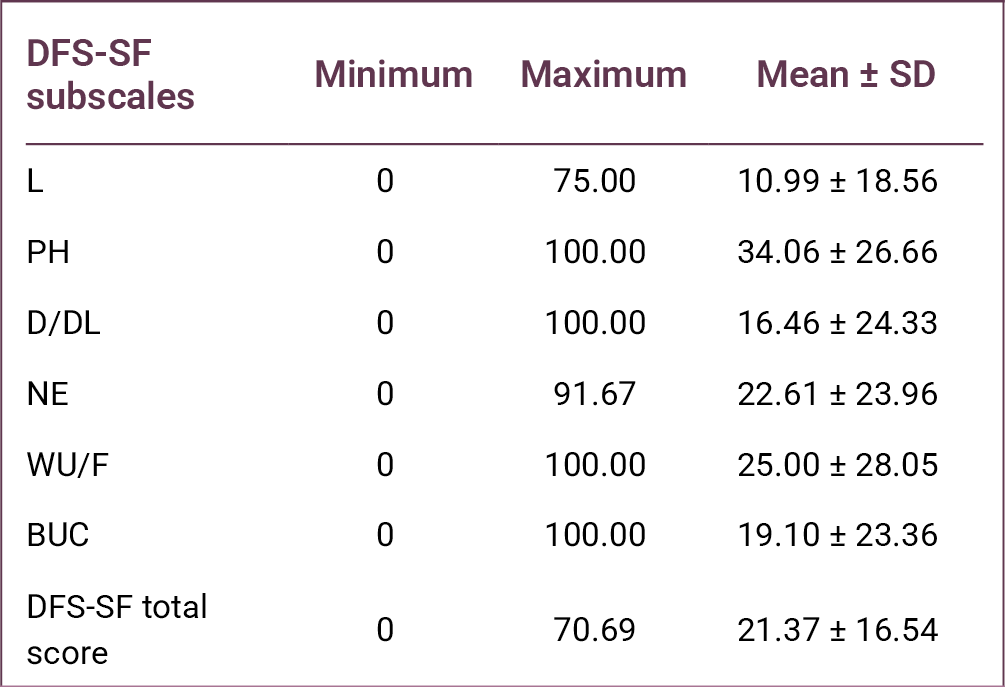
The mean DFS-SF total score was 21.37 ± 16.54, indicating substantially impaired HRQoL among patients with DFUs. Among the DFS-SF subscales, the highest mean score was observed in PH (34.06 ± 26.66), followed by WU/F (25.00 ± 28.05) and NE (22.61 ± 23.96). The lowest score was observed in the L subscale (10.99 ± 18.56) (Table 2).
When DFS-SF scores were analyzed according to sociodemographic characteristics, a statistically significant difference in total DFS-SF scores was found according to educational level (p = 0.036). Among the subscales, only the WU/F score differed significantly across educational groups (p = 0.015). Post-hoc Tukey analysis revealed that participants with primary school education had higher WU/F scores compared to literate individuals.
Significant differences were also observed according to place of residence, with differences detected in NE scores (p < 0.001) and DFS-SF total scores (p = 0.006). Similarly, urbanization level was associated with significant differences in NE, WU/F, and DFS-SF total scores (p = 0.018, p = 0.002, and p = 0.010, respectively).
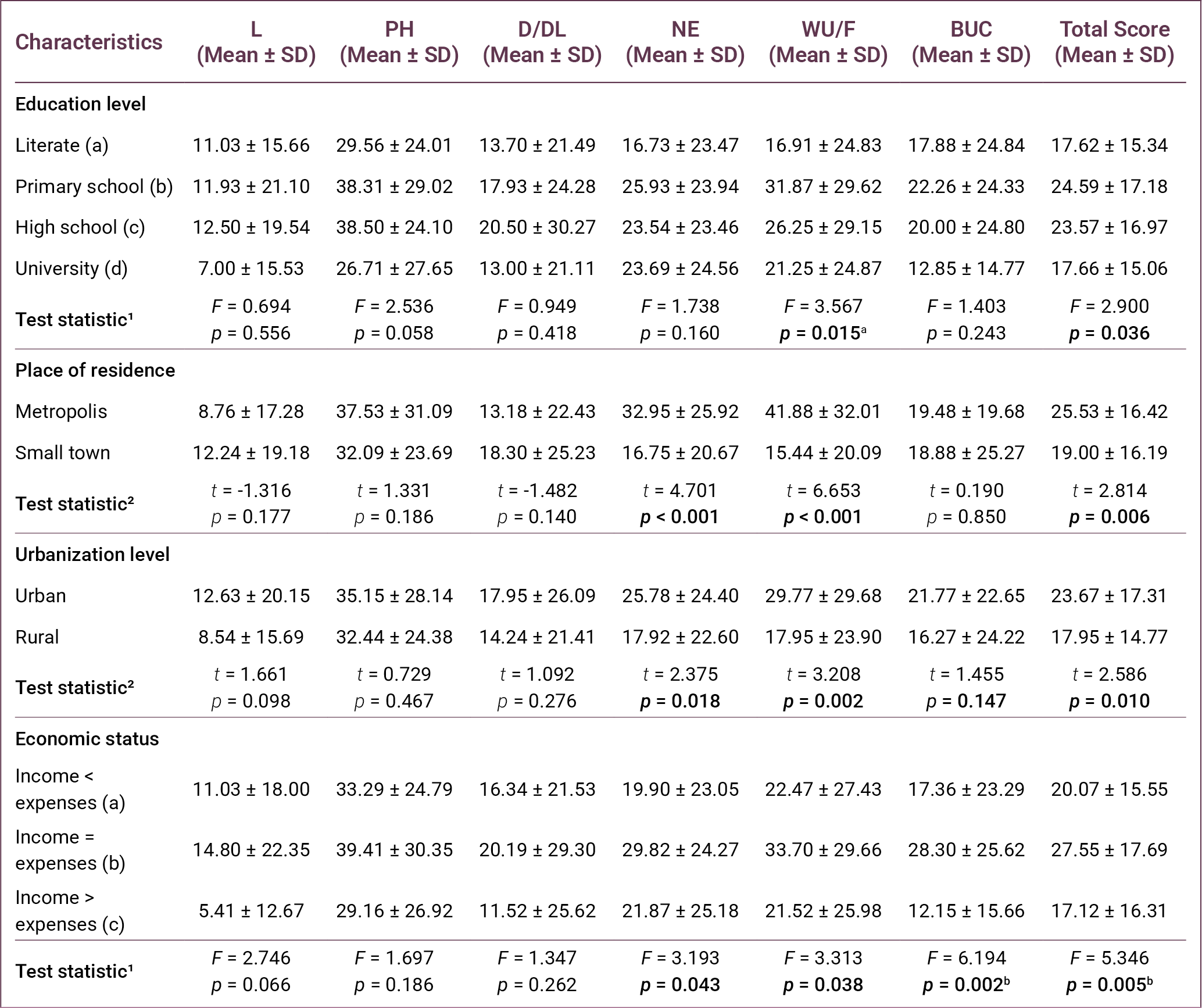
Regarding economic status, statistically significant differences were found in NE, WU/F, bothered by ulcer care (BUC), and total DFS-SF scores (p = 0.043, p = 0.038, p = 0.002, and p = 0.005, respectively). Post-hoc analysis demonstrated that participants whose income equaled their expenses had higher WU/F and BUC scores compared with those whose income exceeded their expenses. Additionally, participants whose income equaled their expenses had higher total DFS-SF scores than those whose income was lower than their expenses (Table 3).
As presented in Table 4, comparisons based on treatment setting showed significant differences in L, NE, WU/F, and BUC scores (p = 0.001, p = 0.004, p < 0.001, and p = 0.042, respectively). Patients without nephropathy demonstrated significantly higher scores in PH, NE, WU/F, and total DFS-SF scores (p = 0.033, p = 0.023, p < 0.001, and p = 0.002, respectively).
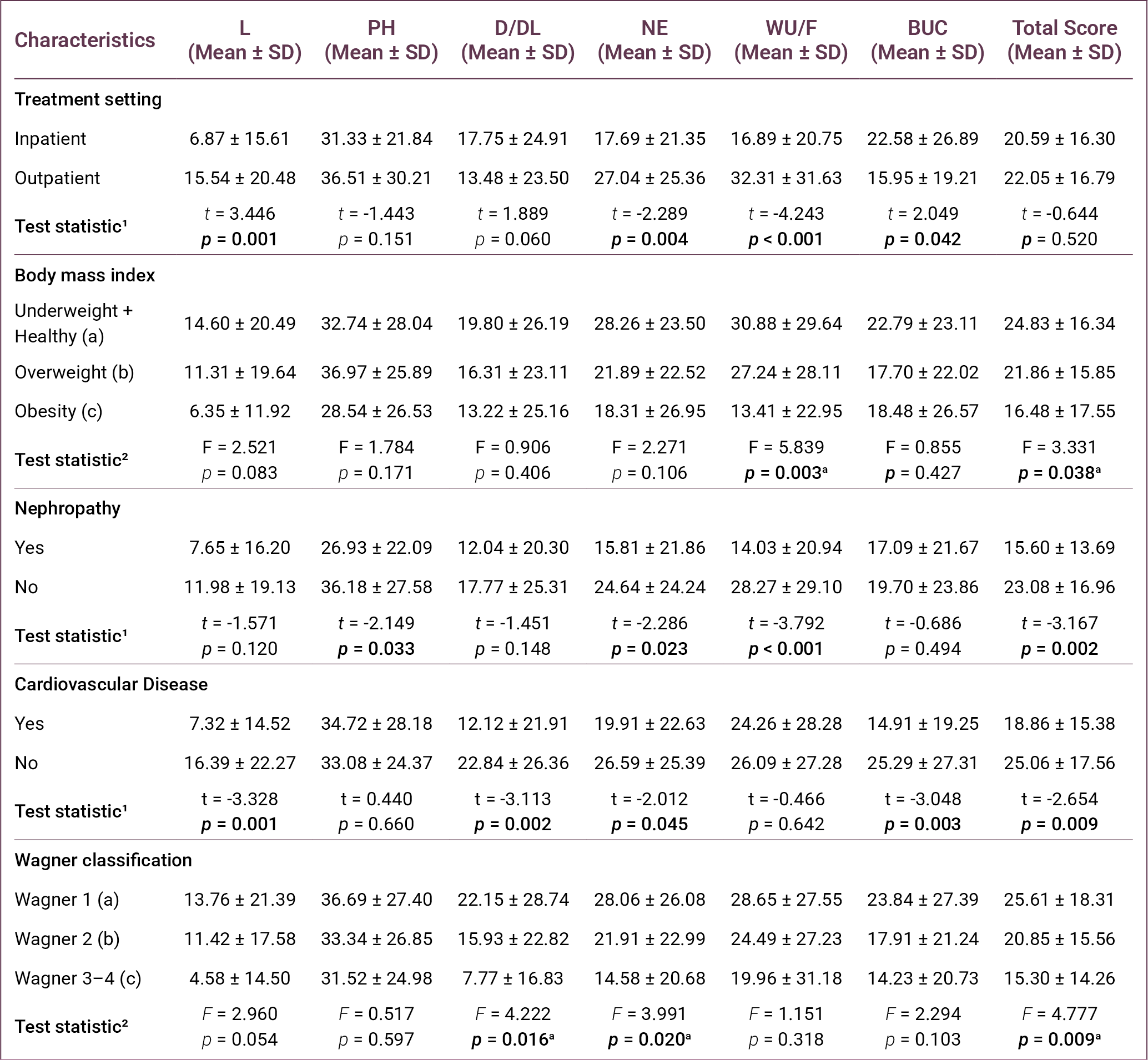
With respect to cardiovascular disease, significant differences were observed in L, D/DL, NE, BUC, and DFS-SF total scores (p = 0.001, p = 0.002, p = 0.045, p = 0.003, and p = 0.009, respectively).
According to the Wagner classification, statistically significant differences were found in D/DL, NE, and total DFS-SF scores (p = 0.016, p = 0.020, and p = 0.009, respectively). Post-hoc Tukey analysis indicated that patients in Wagner stage 1 ulcers had higher scores compared to those with stages 2 and 3–4.
As presented in Table 5, comparisons according to ulcer- and symptom-related characteristics showed statistically significant differences in WU/F and BUC scores according to a history of DFUs (p = 0.002 and p = 0.011, respectively).
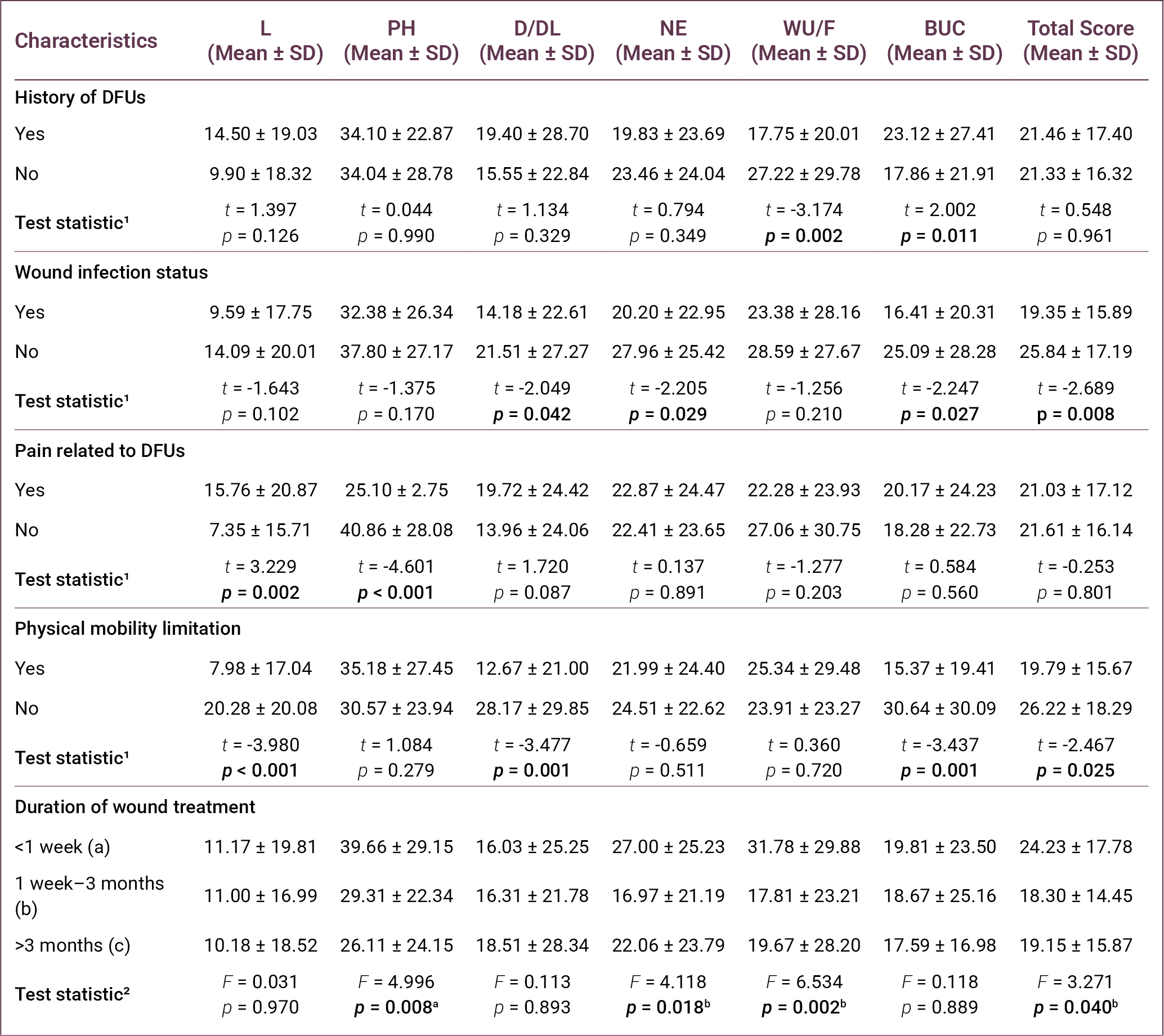
Significant differences were also observed in D/DL, NE, BUC, and total DFS-SF scores according to the presence of wound infection (p = 0.042, p = 0.029, p = 0.027, and p = 0.008, respectively).
In terms of pain related to DFUs, significant differences were found in L and PH scores (p = 0.002 and p < 0.001, respectively). Similarly, physical mobility limitation was associated with significant differences in L, D/DL, BUC, and total DFS-SF scores (p < 0.001, p = 0.001, p = 0.001, and p = 0.025, respectively).
Regarding duration of wound treatment, statistically significant differences were found in PH, NE, WU/F, and DFS-SF total scores ( p = 0.008, p = 0.018, p = 0.002, and p = 0.040, respectively). Post-hoc analysis indicated that participants with wound durations of less than 1 week had higher scores than those with longer wound durations.
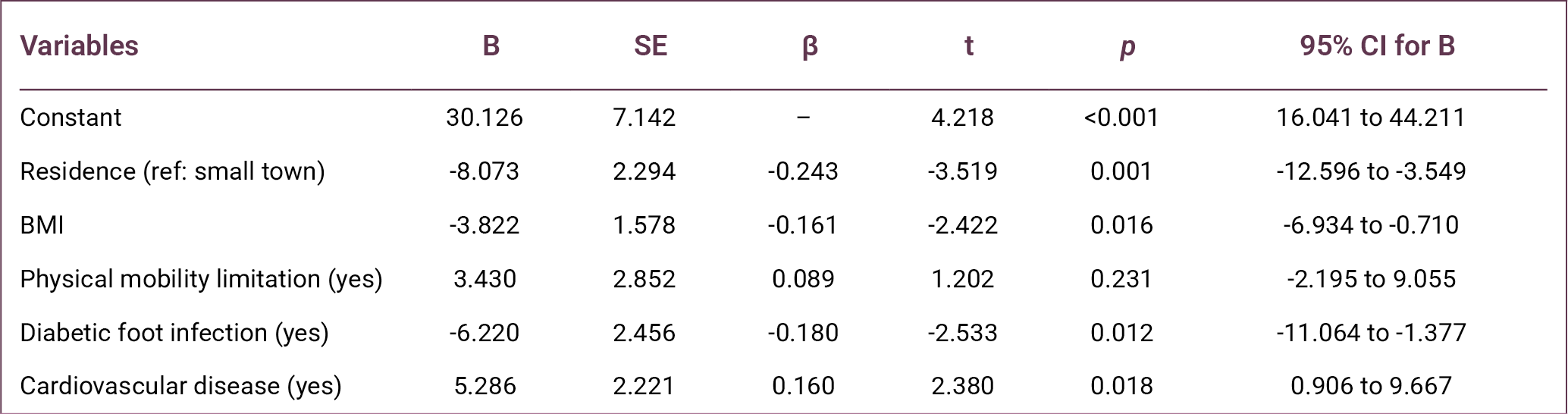
Finally, multivariate linear regression analysis was performed to identify independent factors associated with the DFS-SF total score. The regression model was statistically significant (F = 7.390, p < 0.001) and explained 15.8% of the variance in the DFS-SF total score (R² = 0.158).
The analysis revealed that place of residence (β = -0.243, p = 0.001), BMI (β=-0.161, p = 0.016), presence of diabetic foot infection (β=-0.180, p = 0.012), and presence of cardiovascular disease (β = 0.160, p = 0.018) were independent factors associated with the DFS-SF total score (Table 6).
Discussion
This study demonstrated that HRQoL is markedly impaired in individuals with DFUs, indicating that DFUs represent not only a clinical condition but also a multidimensional burden affecting physical, functional, and psychosocial domains. The low DFS-SF scores observed across all subscales, particularly in L and D/DL, highlight the substantial restrictions imposed by the disease on patients’ everyday functioning.
A prospective cohort study conducted in Singapore reported that HRQoL was low at baseline in patients with DFUs, with an EuroQol 5-Dimension (EQ-5D) utility value of 0.736 (9). Similarly, the Eurodiale study demonstrated that quality of life in patients presenting with DFUs was significantly affected, particularly in the areas of mobility and pain/discomfort (10). In a study conducted by Lima Neto et al. (16) in Brazil, scores on most subscales of the SF-36 quality of life questionnaire were reported to be low in individuals with DFUs, with the “physical role limitations” domain being the most affected. Likewise, Sekhar et al. (11) showed that both physical and mental quality-of-life scores were significantly lower in patients with DFUs compared with individuals without diabetic foot. Furthermore, a meta-analysis involving adults with DFUs reported markedly lower quality of life, particularly in the domains of physical functioning, physical role, general health, and vitality (7). Together, these findings consistently demonstrate that DFUs negatively affect quality of life across multiple dimensions.
In the present study, the relatively low quality-of-life scores may be explained by the clinical characteristics of the study population. A considerable proportion of participants experienced mobility limitation (75.6%), wound infection (69.0%), and DFU-related pain (43.2%), all of which are known to negatively affect physical functioning and daily activities. Additionally, the relatively high mean age of the participants (61.59 ± 12.48), with approximately 40% aged ≥65 years, may have contributed to the lower HRQoL observed. Advanced age is often associated with increased comorbidity burden, reduced physical capacity, and delayed wound healing, which may lead to a greater impact on quality of life in patients with DFU (8,17).
Consistent with previous studies, ulcer severity emerged as a key determinant of HRQoL in this study. The progressive decline in quality-of-life scores with increasing Wagner stage suggests that disease progression is closely linked to worsening functional status and symptom burden. Advanced-stage ulcers are typically associated with higher infection risk, prolonged treatment duration, and increased likelihood of hospitalization or amputation, all of which may impair patients’ physical and psychological well-being.
Similar findings have been reported in previous research. Alrub et al. (18) demonstrated that patients with lower Wagner stages reported significantly higher quality-of-life scores. Likewise, Kudlová and Kočvarová (8) reported that ulcer depth and clinical severity are associated with quality of life in individuals with DFUs. A systematic review examining the impact of diabetic foot complications also concluded that advanced-stage ulcers cause more pronounced deterioration in quality of life (19). Furthermore, a meta-analysis of DFU studies reported that larger wounds were associated with a significant decline in quality of life (7). These findings support the notion that ulcer severity is one of the key clinical indicators determining quality of life in patients with DFUs.
Mobility limitation was another critical factor associated with poorer HRQoL. A large proportion of participants experienced restricted physical movement, suggesting that loss of independence is a central component of the disease burden in DFUs. Reduced mobility may limit participation in daily and social activities, thereby negatively affecting both physical and emotional aspects of quality of life. Previous research also highlights the importance of mobility in determining HRQoL. The Eurodiale study reported that inability to walk or dependence on others for daily activities was associated with a marked decline in quality of life across many domains (10). Similarly, studies have shown that mobility limitations negatively affect physical functioning and activities of daily living in patients with diabetic foot problems (16,20,21). These findings highlight the importance of incorporating rehabilitation strategies and mobility-preserving interventions into DFU management.
This study also highlights the role of clinical complications, particularly infection and comorbid conditions. Diabetic foot infection was identified as an independent predictor of lower HRQoL, likely reflecting its association with pain, inflammation, and treatment complexity. Similarly, the presence of cardiovascular disease was associated with reduced quality of life, possibly due to decreased physical capacity and increased overall disease burden.
Multivariate regression analysis identified place of residence, BMI, diabetic foot infection, and cardiovascular disease as independent predictors of quality of life. In particular, place of residence was found to be one of the strongest predictors (β = -0.243, p = 0.001). This finding indicates that HRQoL in patients with diabetic foot disease is influenced not only by clinical factors but also by socioeconomic and environmental conditions, such as access to healthcare services, availability of social support, and healthcare infrastructure (21).
Individuals living in large cities had lower quality-of-life scores in this study. This finding may reflect differences in living conditions, the burden of disease, social support networks, and access to healthcare services in large cities. However, this finding needs to be clarified by further studies. Furthermore, lower educational and economic status were associated with poorer quality of life, which may be explained by differences in health literacy, self-care behaviors, and access to healthcare resources (13).
Body mass index was also negatively associated with HRQoL (β = -0.161, p = 0.016). Higher BMI may worsen outcomes in patients with DFUs through mechanisms such as reduced mobility, increased plantar pressure, delayed wound healing, and difficulties in implementing effective off-loading strategies (7). Consequently, obesity may exacerbate both ulcer formation and the wound-healing process while simultaneously limiting physical functioning and independence. These findings underscore the importance of integrating weight management strategies into comprehensive DFU care.
Diabetic foot infection was also identified as an independent determinant of HRQoL (β = -0.180, p = 0.012). Infection may negatively affect patients’ physical and psychosocial well-being through pain, inflammation, prolonged treatment duration, and increased need for hospitalization (22). Similarly, the decisive role of infection on quality of life is also emphasized in the literature (10,23). Consequently, early diagnosis and effective management of infection are essential not only for clinical recovery but also for preserving patients’ quality of life.
The presence of cardiovascular disease was identified as an independent determinant of quality of life. Cardiovascular diseases can negatively affect quality of life in patients with diabetic foot through mechanisms such as peripheral circulatory disorders, reduced physical capacity and functional limitations (14,23). The fact that cardiovascular diseases reduce physical capacity and lead to functional limitations may contribute to a decline in quality of life in patients with diabetic foot. Furthermore, the identification of the presence of cardiovascular disease as one of the independent determinants of quality of life in the regression analysis in this study supports the importance of this relationship.
Although the regression model explained a modest proportion of variance in HRQoL, this finding suggests that additional psychological, behavioral, and healthcare-related factors may also contribute to patient outcomes. Nevertheless, the predictors identified in this study provide clinically relevant targets for intervention.
Overall, these findings indicate that improving HRQoL in patients with DFUs requires a comprehensive and multidisciplinary approach. Beyond wound care, effective management should include infection control, management of comorbidities, mobility support, and attention to socioenvironmental determinants of health. Such integrated care strategies may enhance both clinical outcomes and patient-reported quality of life.
This study has several limitations. First, the cross-sectional design limits the ability to establish causal relationships between variables. Second, the sample was recruited from two healthcare centers, which may limit the generalizability of the findings. Third, quality of life was assessed using self-reported measures, which may introduce response bias. In addition, the cross-sectional design did not allow evaluation of longitudinal changes in HRQoL over time. Despite these limitations, the inclusion of participants from two different clinical centers enhances the clinical relevance of the findings. Future multicenter and longitudinal studies are needed to better understand the determinants of HRQoL in patients with DFUs.
In conclusion, this study demonstrates that HRQoL is generally impaired among individuals with DFUs and is influenced by both clinical and sociodemographic factors. Ulcer severity, diabetic foot infection, mobility limitations, BMI, and comorbid cardiovascular disease were associated with poorer HRQoL, while place of residence emerged as an important socioenvironmental determinant. Our findings highlight the multidimensional burden of DFUs and emphasize the need for early identification and management of modifiable risk factors. Further longitudinal research is needed to better understand the long-term impact of these interventions on quality of life.
REFERENCES
GBD 2021 Diabetes Collaborators. Global, regional, and national burden of diabetes from 1990 to 2021, with projections of prevalence to 2050: a systematic analysis for the Global Burden of Disease Study 2021. Lancet. 2023;402(10397):203–34. Erratum in: Lancet. 2023;402(10408):1132. Erratum in: Lancet. 2025;405(10474):202. [CrossRef]
International Diabetes Federation. IDF annual report 2024 [Internet]. Brussels: International Diabetes Federation; 2024. [cited March 24, 2026]. Available from: https://idf.org
Armstrong DG, Tan TW, Boulton AJM, Bus SA. Diabetic foot ulcers: a review. JAMA. 2023;330(1):62–75. [CrossRef]
Armstrong DG, Swerdlow MA, Armstrong AA, Conte MS, Padula WV, Bus SA. Five year mortality and direct costs of care for people with diabetic foot complications are comparable to cancer. J Foot Ankle Res. 2020;13(1):16. [CrossRef]
Schaper NC, van Netten JJ, Apelqvist J, Bus SA, Fitridge R, Game F, et al; IWGDF Editorial Board. Practical guidelines on the prevention and management of diabetes-related foot disease (IWGDF 2023 update). Diabetes Metab Res Rev. 2024;40(3):e3657. [CrossRef]
Navarro-Flores E, Cauli O. Quality of life in ındividuals with diabetic foot syndrome. Endocr Metab Immune Disord Drug Targets. 2020;20(9):1365–72. [CrossRef]
Khunkaew S, Fernandez R, Sim J. Health-related quality of life among adults living with diabetic foot ulcers: a meta-analysis. Qual Life Res. 2019;28(6):1413–27. [CrossRef]
Kudlová P, Kočvarová I. Quality of life in patients with diabetic foot ulcers. Cent Eur J Nurs Midw. 2020;11(1):34–42. [CrossRef]
Lam BJW, Lee PYF, Liew H, et al. Health-related quality of life of patients with diabetic foot ulcers in Singapore: A cross-sectional and longitudinal analysis. Proc Singap Healthc. 2025;34. [CrossRef]
Siersma V, Thorsen H, Holstein PE, Kars M, Apelqvist J, Jude EB, et al. Health-related quality of life predicts major amputation and death, but not healing, in people with diabetes presenting with foot ulcers: the Eurodiale study. Diabetes Care. 2014;37(3):694–700. [CrossRef]
Sekhar MS, Thomas RR, Unnikrishnan MK, Vijayanarayana K, Rodrigues GS. Impact of diabetic foot ulcer on health-related quality of life: A cross-sectional study. Semin Vasc Surg. 2015;28(3-4):165–71. [CrossRef]
Kuman Tunçel Ö, Mert M, Erdem HA, Öztürk AM, Vahabi A, Şanlıdağ G, et al. [The quality of life in the patients with diabetic foot ulcers]. FLORA. 2021;26(2):295–302. Turkish. [CrossRef]
Kolarić V, Svirčević V, Bijuk R, Zupančič V. Chronic complications of diabetes and quality of life. Acta Clin Croat. 2022;61(3):520–7. [CrossRef]
Bann CM, Fehnel SE, Gagnon DD. Development and validation of the Diabetic Foot Ulcer Scale-short form (DFS-SF). Pharmacoeconomics. 2003;21(17):1277–90. [CrossRef]
Kiliç M, Karadağ A, Koçakgöl N. The validity and reliability of the Diabetic Foot Scale-Short Form (DFS-SF) in the Turkish population: a methodological study. Turk J Med Sci. 2023;53(5):1438–47. [CrossRef]
Lima Neto PM, Lima PHS, Santos FDRP, Jesus LMS, Lima RJCP, Santos LH. Quality of life of people with diabetic foot. Rev Rene. 2016;17(2):191–7. [CrossRef]
Nemcová J, Hlinková E, Farský I, Žiaková K, Jarošová D, Zeleníková R, et al. Quality of life in patients with diabetic foot ulcer in Visegrad countries. J Clin Nurs. 2017;26(9-10):1245–56. [CrossRef]
Alrub AA, Hyassat D, Khader YS, Bani-Mustafa R, Younes N, Ajlouni K. Factors associated with health-related quality of life among Jordanian patients with diabetic foot ulcer. J Diabetes Res. 2019;2019:4706720. [CrossRef]
Eroğlu N. [Diabetic foot problems in diabetic patients effect on quality of life: systematic review]. J Nurs Sci. 2018;1(2):19–22. Turkish.
Sothornwit J, Srisawasdi G, Suwannakin A, Sriwijitkamol A. Decreased health-related quality of life in patients with diabetic foot problems. Diabetes Metab Syndr Obes. 2018;11:35–43. [CrossRef]
Stasini FB, Margari N, Fasoi G, Kelesi M, Dafogianni C. Quality of life among patients with diabetic foot ulcer. Int J Caring Sci. 2020;13(2):1073–80.
Raspovic KM, Wukich DK. Self-reported quality of life and diabetic foot infections. J Foot Ankle Surg. 2014;53(6):716–9. [CrossRef]
Oe M, Saad SS, Jais S, Sugama J. Impact of foot ulcer-related factors on quality of life in patients with diabetes: Prospective observational study. Int Wound J. 2024;21(5):e14895. [CrossRef]